Ischemic stroke can be caused by various mechanisms, and prevention of recurrent ischemic stroke is dependent on the recognition of the accurate mechanism of cerebral infarction. However, unfortunately, an underlying stroke mechanism is not identified in many patients with ischemic stroke despite the patients undergoing diagnostic evaluations.1 In particular, embolic stroke of undetermined source (ESUS), which accounts for approximately 20% of strokes, suggests various etiologies, including paroxysmal atrial fibrillation, occult malignancy, atrial cardiomyopathy, or nonsignificant stenotic atherosclerotic plaque.1 Usually, more than 50% relevant artery stenosis is regarded as significant and may be responsible for an ischemic lesion in the corresponding brain area.2 However, when nonsignificant stenosis of the relevant artery is observed in the diagnostic evaluation, additional workups to detect the cardioembolic source or coagulopathies are usually performed.
Here, we report a case of embolic infarction without significant stenosis at the proximal carotid artery that was evaluated by magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA), and a mobile thrombus with an ulcerative plaque was observed by carotid duplex ultrasonography and was confirmed by digital subtraction angiography (DSA). Our case may show the usefulness of carotid ultrasonography in patients who have ischemic stroke with an embolic pattern without significant arterial stenosis.
CASE
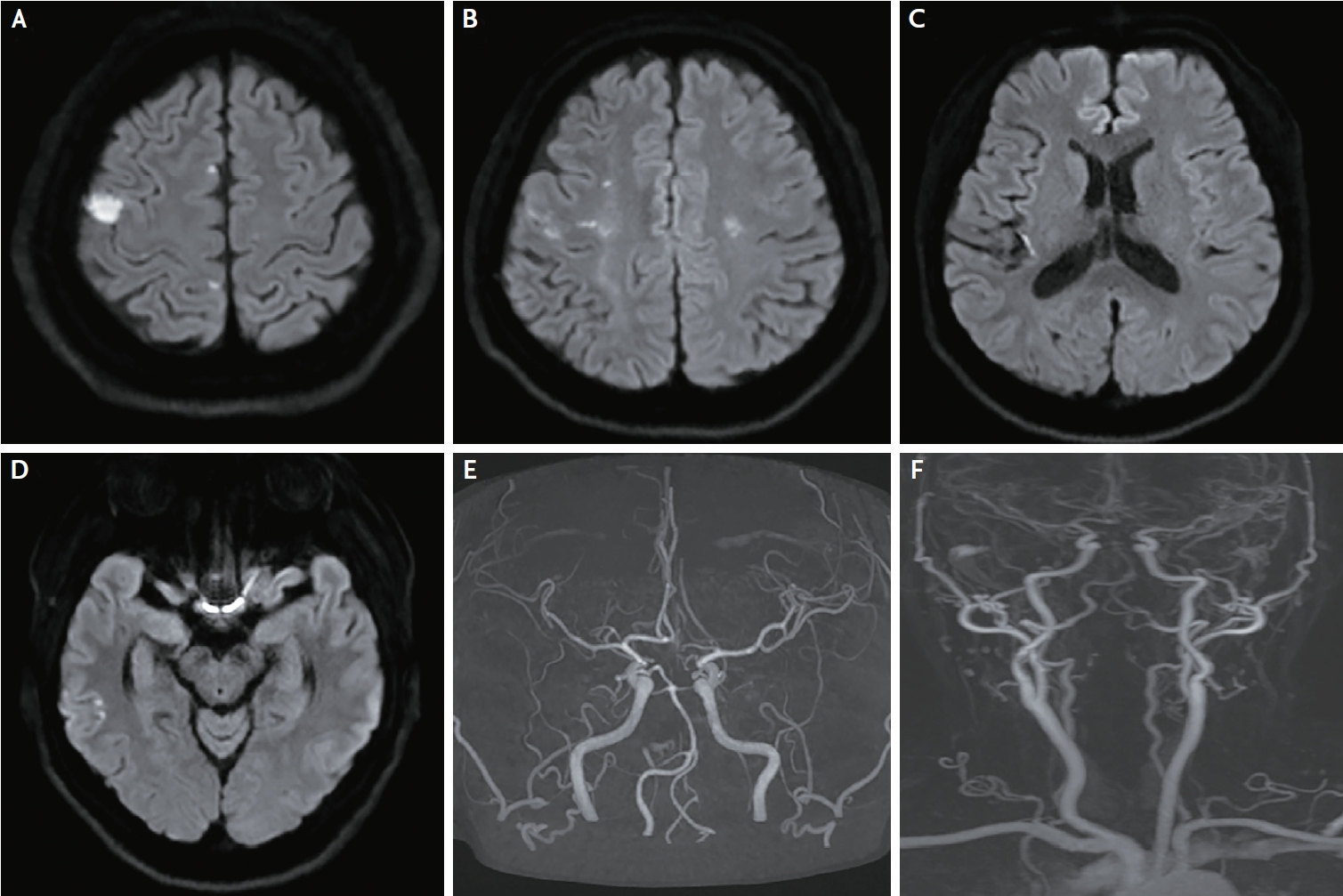
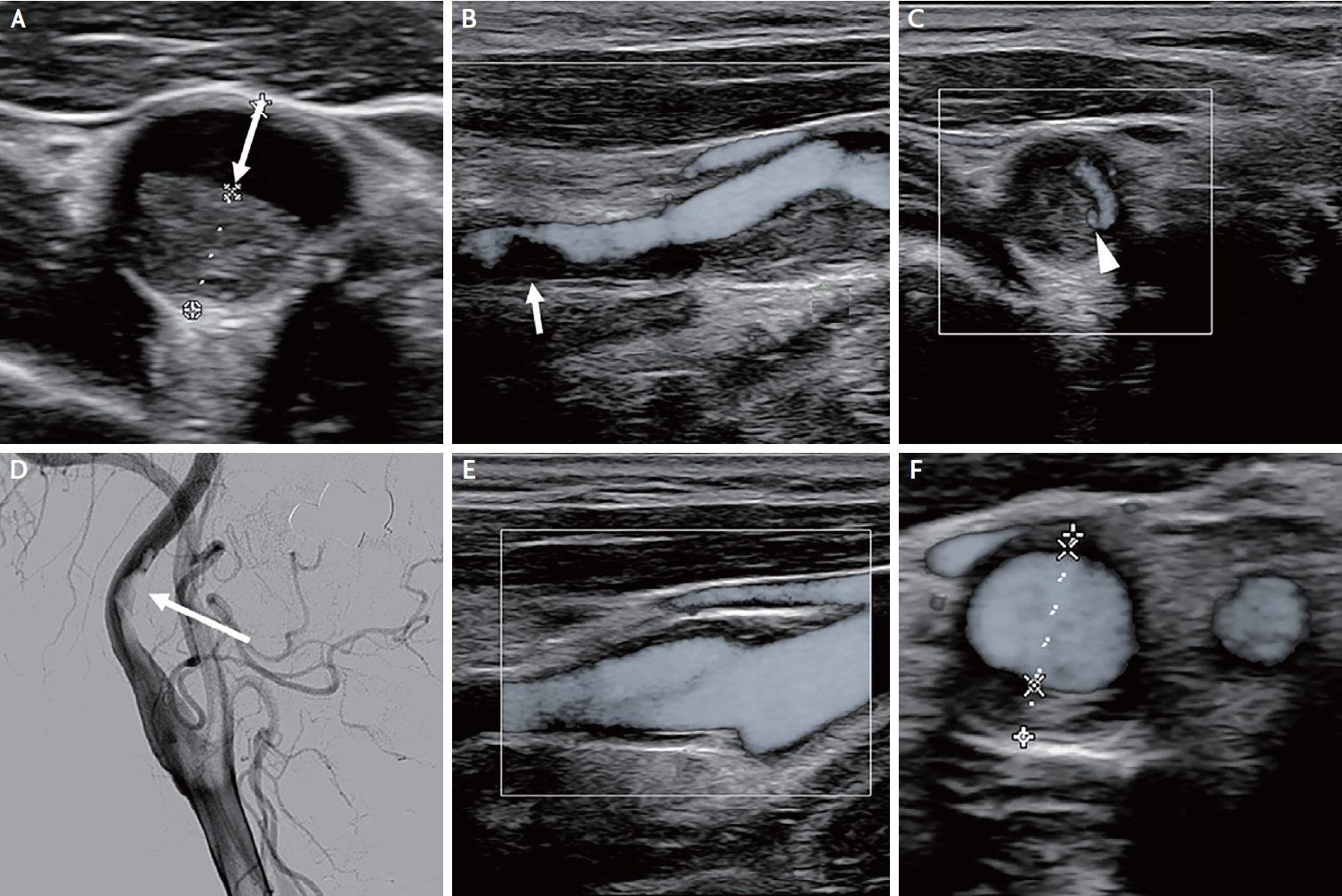
A 53-year-old woman presented with sudden-onset dysarthria and motor weakness of the left limb, which occurred three days prior. The patientŌĆÖs blood pressure measured at the emergency center was 130/80 mmHg, and the patientŌĆÖs pulse rate was 62 beats/min. Her baseline National Institutes of Health Stroke Scale was 3. She did not have any cardiovascular risk factors, family history of cardiovascular disease, or symptoms suggesting connective tissue disorders. Electrocardiography revealed a sinus rhythm. Brain MRI and MRA revealed multiple tiny, scattered diffusion-restricted lesions, which were present in the right frontal, temporal, insular cortex and left frontal cortex (Fig. 1A-D), and there were nonsignificant stenotic lesions in the intracranial or extracranial arteries (Fig. 1E, F). Initial blood test results, including tests for infection, vasculitis, coagulopathy, and inflammation markers, were within the reference ranges. Transthoracic echocardiography revealed normal left ventricle systolic function (ejection fraction: 57%) and no significant valvular disease. There was no evidence of common etiologies of cryptogenic stroke, such as paroxysmal atrial fibrillation on Holter monitoring, patent foramen ovale on transcranial Doppler monitoring and transesophageal echocardiography, or aortic arch atheroma and obstructive coronary artery disease on cardiac computed tomography (CT) angiography. We initially considered the insertion of a loop recorder device. However, carotid duplex ultrasonography showed a mobile thrombus with an ulcerative plaque, which was confirmed as a ruptured and mobile thrombus through subsequent DSA (Fig. 2A-D). We did not insert a loop recorder device and decided to treat the patient with aspirin (100 mg/day), clopidogrel (75 mg/day) and high-dose statins. The patient maintained dual antiplatelet treatment with high-dose statins, and at the follow-up carotid duplex ultrasonography 6 months after stroke onset, the mobile plaque had disappeared (Fig. 2E, F).
DISCUSSION
The current case shows a patient with ischemic stroke that occurred at the scattered cortical infarction in the right internal carotid artery (ICA) and left anterior cerebral artery (ACA) vascular territory. No significant stenosis was observed on contrast-enhanced MRA. Additionally, a cardioembolic source or coagulopathy was not observed in the diagnostic evaluation. We initially considered insertion of a loop recorder device. However, carotid duplex ultrasonography showed a mobile thrombus with an ulcerative plaque, which was confirmed as a ruptured and mobile thrombus through DSA. We did not insert a loop recorder device and decided to treat the patient with dual antiplatelets and high-dose statins.
In the global ESUS registry, 79% of ESUS patients had some degree of nonstenotic ICA plaques.3,4 This finding suggested that the presence of a carotid plaque is extremely common. However, nonstenotic carotid plaques might be considered an incidental finding in many cases and might not have been the source of the stroke. The presence of carotid plaque is considered as a possible cause of stroke according to the Trial of ORG 10172 in Acute Stroke Treatment, but only if stenosis >50% is present (large artery atherosclerosis). The 50% threshold was derived from clinical trials of carotid endarterectomy, in which carotid endarterectomy was effective in preventing future stroke among patients with carotid stenosis >50%.5 Therefore, a lesion with less than 50% stenosis with a carotid plaque is classified as ESUS and might be underestimated as a potential source of stroke.
Determining whether a nonstenotic carotid plaque is the stroke mechanism in an individual patient is a major challenge. A previous study showed that a similar prevalence of nonstenotic carotid plaques was observed for studies that used ultrasound, CT angiography and MRA (46-59%). However, the prevalence in studies using DSA was lower (30%).6 These limitations might have led to underrecognition of nonstenotic carotid plaques. In the present case, we did not even observe significant stenosis on the contrast-enhanced MRA. However, a mobile thrombus with an ulcerative plaque was observed by carotid duplex ultrasonography and was confirmed by DSA. Furthermore, a previous study showed that large (Ōēź3 mm thick) but nonstenotic carotid artery plaques are more common in cryptogenic stroke.4 Additionally, ipsilateral vulnerable nonstenotic carotid plaque and plaque surface irregularity are associated with ESUS in anterior circulation infarctions. In the current case, a large thrombus (4.7 mm thick) and an ipsilateral vulnerable (hypoechoic) nonstenotic carotid plaque were observed. Additionally, the cerebral blood flow of the left ACA territory was supplied through the right ACA A1 and anterior communicating artery because the patient had asymmetry and hypoplasia of the left ACA A1. Because no other stroke causes were present, a nonstenotic (<50%) carotid plaque with highrisk features (ulcerative plaque) was observed on ultrasound and DSA, the acute embolic stroke was confined to the corresponding ICA territory on diffusion-weighted imaging, and the absence of acute or chronic infarcts in other vascular territories was confirmed,7 we thought that our case was diagnosed as nonstenotic carotid disease.
The optimal treatment strategy for patients with ESUS remains unclear because it is difficult to determine the main cause of ESUS. A recent study showed that atrial fibrillation is more commonly detected among ESUS patients without carotid plaque, and the RESPECT-ESUS trial found a possible benefit to oral anticoagulation in older but not younger subjects.8 However, another study showed that anticoagulation is no more effective than antiplatelet therapy in unselected ESUS patients.9 In a subgroup analysis of the POINT trial, dual antiplatelet therapy provided a statistically nonsignificant reduction in recurrent ischemic stroke with no difference in the safety outcomes compared to aspirin monotherapy in patients with minor ischemic stroke associated with ipsilateral nonstenotic carotid disease.10
In conclusion, for patients with an embolic lesion pattern restricted to a single vascular territory, evaluation by carotid duplex ultrasonography may be beneficial for finding a potential artery-to-artery embolic source, even in patients with symptomatic nonstenotic carotid artery disease.