INTRODUCTION
Stroke is the second most common cause of death worldwide and a significant proportion of all ischemic strokes are due to carotid atherosclerotic disease.1 Carotid atherosclerosis has a high prevalence in Western countries, affecting up to 75% of men and 62% of women aged 65 years and older.2
Currently, and over the last several decades, the reduction in luminal diameter of the extracranial carotid arteries has been considered to be the key parameter for stratifying the severity of carotid artery atherosclerosis. This resulted from the study design of clinical trials conducted during the 1980s to the mid-1990s.3,4 Despite these very important clinical trials, histopathological studies demonstrate that plaques with identical degrees of stenosis can display considerable differences in composition and also in risk of rupture.5
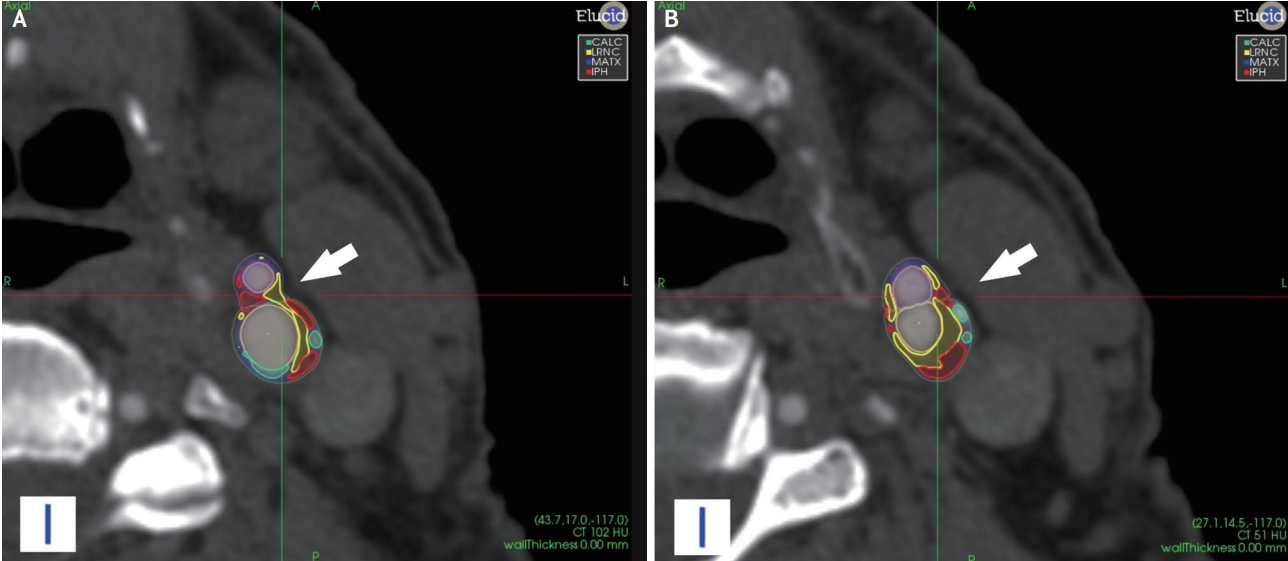
The evolution of computed tomography (CT) and magnetic resonance (MR) imaging techniques has allowed for the routine characterization of carotid plaque features (Figs. 1 and 2). The traditional concept of using the degree of luminal stenosis as the sole imaging marker for the selection of the optimal therapeutic approach is challenged by a rapidly growing body of literature demonstrating that plaques causing only mild stenosis may still lead to stroke.6,7 Moreover, it is important to underline that plaque composition may change dramatically over a few years and cardiovascular risk factors play a major role in these changes.8 Physicians treating patients with carotid disease should be aware of this paradigm shift since nowadays the imaging of vulnerable plaques and their characterization plays a key role towards the improvement of risk stratification and therapy selection in patients with both high- and low-degree carotid artery stenosis.
IMAGING TECHNIQUES AND PLAQUE FEATURES OF VULNERABILITY
The characterization of the carotid artery atherosclerotic wall is the focus of several ongoing research efforts which investigate the optimal approach to the imaging of the vulnerable plaque.9,10 The target of plaque imaging is to look beyond the lumen using advanced wall imaging methods in order to identify the vulnerable plaque.7,11 This is a rapidly evolving field because of the evolution of CT and MR technologies that can provide exquisite, high-resolution imaging of the carotid artery lumen and arterial plaques. Literature5,12 shows that certain plaque features are associated with an increased risk of plaque rupture, including intra-plaque hemorrhage (IPH), thin or ruptured fibrous cap (FC), presence and size of the lipid-rich-necrotic-core (LRNC), and active plaque inflammation. In the following sections the features linked to plaque vulnerability are presented.
1. CT
CT is a non-invasive and widely used technique that allows assessment of the atherosclerotic plaque burden and the degree of stenosis.13-17 Modern CT scanners are able to perform detailed imaging of the carotid artery lumen and of the plaque. Visualization of the vessel lumen is achieved by performing a CTA which requires the injection of an iodinated contrast medium. Because of its excellent spatial resolution, CT imaging is a promising tool for the quantification of the volume of the carotid plaque and its sub-components (fatty – mixed – calcified) and it is potentially able to detect IPH.13,18-20 In particular, the introduction of multi-energy21 technology further increases the capabilities of CT in the detection and characterization of carotid atherosclerosis. Advantages of multi-energy CT compared with conventional CT include the ability to differentiate calcified plaque from iodinated contrast, while also facilitating bone subtraction. Limitations of CT are mainly related to the radiation dose delivered to the patients and to the potential side effects of contrast materials.13,22,23 In the last years, several papers have been published using positron emission tomography (PET)-CT which can identify various functional images.24 For PET, the most commonly used tracer is 18F-fluoro-2-deoxy-D-glucose (18F-FDG). PET-18F-FDG allows the measurement of metabolic activity in atherosclerotic plaques, which correlates with plaque macrophage infiltration and vascular endothelial growth factor. Another tracer introduced is 18F-fluorocholine (18F-FCH). Choline is a precursor of phosphatidylcholine, a key component of all cellular membranes and correlates strongly with degree of macrophage infiltration and recent symptoms.25 Also nanoparticles are being used for molecular imaging of atherosclerosis and in particular iron oxide MRI contrast agents provide highly efficient iron-labeling in macrophages for magnetic resonance-based detection in vivo24 and were reported as very promising in the detection of plaque inflammation.25
2. MR
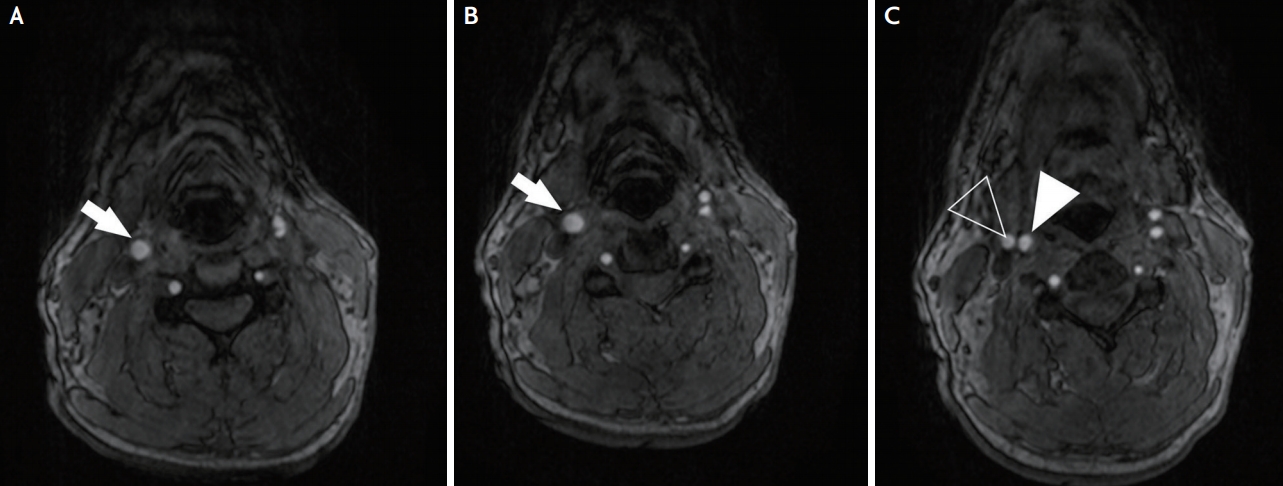
MRI is currently considered the most favorable non-invasive imaging technique (Fig. 3) to characterize features of plaque vulnerability such as intra-plaque hemorrhage IPH, LRNC, and the status of the FC.26
MR allows for the accurate distinction of plaque components27 such as the LRNC, fibrous tissue, and IPH exploiting their different signal properties. While the identification of calcified components can be more challenging compared to CT, MR still offers usually good results. MR plaque imaging is usually combined with an MR angiography which provides information about the luminal morphology, including plaque ulceration. This can be either a time-of-flight MRA, which does not require the injection of a contrast medium, or a contrast-enhanced MRA, which is acquired during the first pass of an i.v. gadolinium bolus.
It is noteworthy that initial research in carotid plaque MR imaging relied on carotid surface coils to provide high-resolution images of the plaque and vessel wall. This was initially considered a limitation because of the lack of availability of such coils in routine clinical practice and the challenges related to adequate positioning of carotid surface coils due to their small coverage.28 However, recently published studies using 3T MRI scanners with conventional neurovascular coils showed promising results in terms of identifying LRNC and IPH,28 even though further data with bigger populations are necessary to corroborate these findings. Drawbacks of MR are the relatively long study times and the sensitivity of image quality to motion effects.
Advanced MR protocols including dynamic contrast enhancement (DCE) allow quantification of plaque vascularity by using gadolinium contrast agents together with pharmacokinetic modeling.29 Moreover, the use of artificial intelligence (AI) algorithms is allowing to improve the general performances.30,31
CAROTID PLAQUE FEATURES OF VULNERABILITY
1. Carotid artery plaque thickness and length
Maximum wall thickness (MWT) represents the maximum thickness of the plaque. This feature can be quantified by US, CT and MRI and is associated with features of plaque vulnerability, such as IPH and status of the FC.32 In a study published in 2017, based on 1,072 symptomatic subjects that underwent MRI of carotid arteries, the MWT was more strongly associated with cerebral ischemic symptoms (AUC=0.93; 95% confidence interval [CI]: 0.91–0.95) than was the degree of stenosis (AUC=0.81; 95% CI: 0.76–0.84).33 The use of advanced techniques34,35 in MR imaging allow to better define the carotid plaque with subsequent plaque thickness quantification.
Another parameter that is simple to characterize on CT and MRI is plaque length. Plaque length does not appear to relate directly to the occurrence of cerebrovascular events, but it is an independent risk factor for peri-procedural complications and excessive re-stenosis rate in carotid interventions.36
2. Surface morphology
The morphology of the luminal surface of carotid plaques is considered a risk feature of cerebrovascular events.3 In particular, the presence of ulceration (Fig. 4) significantly increases the risk of cerebrovascular events. Conventional US is generally not considered an optimal technique for the detection of irregular plaque surface and ulcerations, but 3D US and CEUS have recently proved effective for this purpose.37 CT and MR offer very good results in detecting ulcerations when compared to histopathology, with performance significantly superior to that of US.38
3. IPH
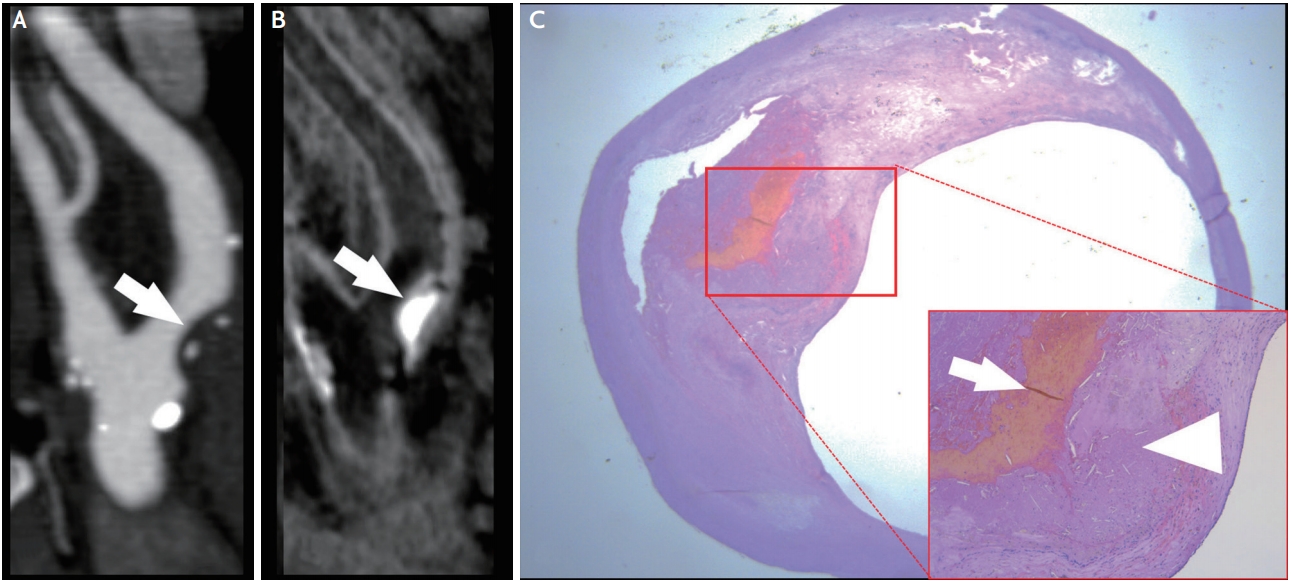
Nowadays IPH is considered one of the identifying features of vulnerable plaque39,40 and several meta-analyses indicate that MRI detection of carotid IPH is associated with increased risk for future ischemic cerebrovascular events in patients with carotid stenosis.41 Among all available imaging techniques, MRI is preferred (Fig. 5) for the detection of IPH because its imaging depends on the oxidative state of hemoglobin,30 which is easily detected on MR via common imaging protocols (e.g T1-MPRAGE or T1-turbo spin echo with fat saturation).18 It is worth noting that dedicated carotid wall imaging with small field-of-view (FOV) surface coils are not needed for the detection of IPH, since this can be achieved at lower spatial resolution using large FOV neck coils.28 CT shows conflicting results in the literature, with some authors going as far to suggest that even low Hounsfield unit (HU) values (<25 HU)42 may associate with the presence of IPH.
4. LRNC and FC
Lipids are one of the key components of atherosclerotic plaques and the size of the LRNC in carotid plaques is believed to be predictive of increased risk of a cerebrovascular event.41 A recent study identified a threshold of 40% LRNC as being associated with an increased risk for occurrence of cerebrovascular events.42 A CT versus MRI comparison (Fig. 5) study reported that the best imaging feature for detection of a complicated AHA type VI plaque by MRI was the thickness of the soft plaque component by CT (receiver operator characteristic area under the curve=0.89).43 Both CT and MR can identify the presence of lipid components thanks to lipid-tissue attenuation properties and signal characteristics.
The FC is a layer of fibrous connective tissue which separates the core of the plaque from the arterial lumen. FC alterations (thin or ruptured cap) are considered an important feature of plaque vulnerability.44 An intact FC is associated with a low risk of occurrence of cerebrovascular events whereas a ruptured FC is associated with a high risk of events.44 By considering non-invasive imaging (therefore excluding intravascular ultrasound), MRI is considered the preferred technique to image this feature for the carotid artery, especially with the use of gadolinium.45
5. Plaque activity: inflammation and neovascularization
Inflammation is a key factor in the pathophysiology of atherosclerosis with regard to progression and destabilization of plaques. Compared to stable lesions, rupture-prone or vulnerable plaques typically exhibit inflammation and intra-plaque neovascularization.5 The pro-inflammatory state caused by endothelial cell dysfunction promotes the expression of cellular adhesion molecules and consequently the recruitment of inflammatory cells (mainly macrophages).5 A significant correlation between macrophage plaque infiltration, plaque rupture and ischemic symptoms exists.5,25 Inflammatory cells accumulate in specific areas of the plaque, typically the shoulder or in the FC.
Another important feature is intra-plaque neovascularization. As the plaque size increases, oxygen levels deep within the plaque diminish, and local hypoxia triggers microvessel formation into the intima through breaks in the media. These neovessels are characterized by an immature endothelial lining and may lead to bleeding in the plaque (IPH). Therefore, the degree of intra-plaque neovascularization is linked to the “activity” of the plaque in terms of inflammation and increased risk of neovessel rupture and hemorrhage (IPH).46,47
CEUS and MR are highly correlated in terms of detecting intra-plaque neovascularization. CT can also help with the detection of intra-plaque neovascularization and in its quantification as the amount of contrast enhancement on CT is associated with the extent of neovascularization.48-50
On MRI, enhancement of the carotid plaque after the administration of gadolinium is associated with neovascularization (p<0.001). There is a correlation between the degree of plaque enhancement and the degree of neovascularization.51 DCE-MR permits quantification of plaque vascularity29 and plaque perfusion and it has been shown to give reproducible physiological measurements of the vasa vasorum. However, as mentioned above, one of the main limitations of DCE-MR is that the vessel wall is difficult to image dynamically because of its small size and motion artifacts.
6. Plaque volume and plaque sub-components analysis
The volume of the carotid artery plaque may be associated with vulnerability of the plaque.52 Measurement of this feature is facilitated by recent software packages for volumetric analysis. Recent papers showed that the volume of the carotid artery plaque is associated with the occurrence of cardiovascular events.53 Evidence indicates that increasing plaque volume is associated with an increase in lipid and calcium components.53 Because of the excellent spatial resolution of CT, it is possible to calculate accurately the total plaque volume and also the volume of the sub-components of the plaque according to the attenuation values of the voxels.54 Similarly, MRI proved useful for plaque component volume quantification55 even though the spatial resolution of MRI is lower than that of CT.
IMPLICATIONS FOR PREVENTION AND TREATMENT OF CEREBROVASCULAR EVENTS
On the one hand, the efficacy of carotid revascularization in stroke prevention in symptomatic individuals with 50 to 99% carotid stenosis is documented but, on the other hand, 70 to 80% of symptomatic patients with >50% stenosis will not experience a recurrent stroke at 5 years.56 This group of patients at relatively low risk of recurrent cerebral ischemic events routinely undergo surgical intervention which will often be unnecessary, demonstrating the limitation of the current risk stratification model, based on degree of stenosis alone.57 It has been demonstrated that early initiation of medical therapy after transient ischemic attack (TIA) or minor stroke significantly lowers the risk of stroke recurrence.58 Therefore, identifying patients at risk of stroke despite modern medical therapy has become increasingly important. Nonetheless, the choice of the correct therapy is debated and some guidelines recommend expanding the indications for carotid revascularization in carotid disease. A risk model which takes into account multiple clinical and demographic patient characteristics in addition to the degree of stenosis represents a step forward in identifying patients at risk of stroke. Inclusion of carotid imaging features into such risk models has the potential to further improve the selection of individual patients for treatment.
The impact of plaque imaging is considered in the recently published guidelines and perspectives. In particular, the perspective and guidelines from the American Society of Neuroradiology vessel wall imaging study group and expert consensus recommendations of the American Society of Neuroradiology, released in February 2018,13 focused on the technological implications and impact of the imaging technologies for the carotid plaque imaging. In this document it is suggested that for carotid artery imaging some technological thresholds are necessary, and in particular for the CT at least a 32-detector-row CT scanner whereas for the MR at least a 1.5T with carotid coil or a 3T system (with or without dedicated carotid coil); moreover in order to obtain the necessary level of information by using the MR a minimum set of sequences are needed and are described in the document. In the “guidelines on diagnosis and treatment of peripheral artery disease”, released by the European Society of Cardiology (ESC)58 in March 2018, it is recommended that for asymptomatic patients with a life expectancy >5 years and 60-99% carotid artery stenosis and imaging features associated with increased risk of ipsilateral stroke (IPH or LRNC), carotid artery revascularization should be considered: carotid endarterectomy (CEA) if they are considered “average surgical risk” (class of recommendation: IIa; level of recommendation: B) and carotid artery stenting if they are considered “high risk for CEA” (class of recommendation: IIa; level of recommendation: B). Ongoing trials will provide further evidence on whether carotid plaque imaging identifies patients who benefit from revascularization. The AHA produced a guideline completely dedicated to the management of patients with extracranial carotid and vertebral artery disease in 2011,59 where the key parameters for the choice of the treatment were the stenosis and the presence of absence of cerebrovascular symptoms. However, new updated version is currently ongoing because of the time occurred from the previous one.
CONCLUSION
The identification of protective imaging features in carotid artery plaques represents a future goal for carotid plaque imaging. In the literature, the protective effect of heavily calcified plaque is described; however, a recent study using energy dispersive X-ray microanalysis identified two types of calcium salts in atheromatous plaques, hydroxyapatite and calcium oxalate. The authors showed an association between hydroxyapatite calcification and unstable plaques whereas calcium oxalate calcifications were mainly detected in stable plaques.60 This finding could widen the utilization of multi-energy CT scanners because of their potential to perform spectral analysis and distinguish between the different subtypes of calcifications61 with the potential for further risk stratification.
Plaque volume seems to be a promising parameter related to the risk of recurrent TIA or stroke. In 2018 Lu et al.62 demonstrated that the annual progression of carotid plaque volume is independently associated with recurrent ischemic cerebrovascular events, and this measurement added value to the presence of IPH and FC rupture in terms of predicting future events. Atherosclerotic plaque volume progression and composition can facilitate the rupture of the plaques.52 Therefore, monitoring plaque volume changes may improve our ability to estimate risk and monitor the effect of medical therapy.
Medical therapy with anti-inflammatory drugs and high-dose statin showed very good results in reducing the occurrence of cardio- and cerebro-vascular events. Monitoring the effect of such medical therapy on the plaque, by checking on the progression and regression patterns, could represent a key element in the selection of the optimal therapy, especially in the light of the different plaque risk profiles independent of the degree of stenosis.
It is likely that a strategy combining more than one approach will prove most valuable, as the different approaches are complementary to each other. Future studies comparing different modalities of plaque imaging will be helpful from this perspective.
AI is booming in all areas of business and medicine.63 Recent advances in the field of AI have opened up new avenues for creating novel modeling and predictive methods for clinical use. The recent explosion of imaging data is creating a path for such approaches because of the huge amount of information included in CT and MR imaging datasets. Deep learning may provide the ability to identify patterns of imaging information and improve risk stratification.64
Several prospective studies (ARIC, MESA, PARISK, CAPIAS, CARE-II, CAIN)9,43,57,65-70 are currently ongoing to assess the value of plaque imaging in stroke risk stratification. Ongoing randomized trials comparing best medical therapy alone versus carotid revascularization either select patients (such as ACTRIS) or allow to measure the benefit of revascularization (such as ECST-2) based on carotid plaque MRI or other extended imaging.
Carotid artery plaques are heterogeneous in terms of biology, pathology and vulnerability with different therapeutic implications based on their features. Imaging plays a key role in the evaluation of patients with atherosclerotic carotid disease because it allows for characterization of the plaque structure and composition. Advanced imaging for the characterization of carotid plaque vulnerability can help refine risk stratification and allow for individualization of care. Further evaluation in randomized clinical trials is needed to establish the exact role of plaque imaging in clinical decision-making.