High Erythrocyte Sedimentation Rate is Associated with White Matter Hyperintensity in a Healthy Population
Article information

Abstract
Background
High erythrocyte sedimentation rate (ESR) is related to various metabolic, cardiovascular, and cerebrovascular diseases; however, there is a limited study about its association with subclinical cerebral small vessel diseases (cSVDs). In this study, we evaluated the relationship between ESR and cSVDs in a healthy population.
Methods
We evaluated healthy check-up volunteers between 2006 and 2013. As subtypes of cSVD, we evaluated white matter hyperintensity (WMH), silent brain infarct (SBI), and cerebral microbleeds (CMBs). The WMH volume was rated quantitatively using a computer-assisted semi-automated technique. SBI and CMBs were evaluated qualitatively for presence.
Results
A total of 2,553 participants were evaluated. In multivariable linear regression analysis, ESR (β=0.027, 95% confidence interval [CI]=0.001 to 0.053, p=0.043) was significantly associated with WMH volumes after adjusting for confounders. Age (β=0.046, 95% CI=0.042 to 0.051, p<0.001), hypertension (β=0.187, 95% CI=0.092 to 0.281, p<0.001), and white blood cell counts (β=0.042, 95% CI=0.018 to 0.067, p=0.001) were also closely related to WMH volumes. ESR did not show any statistical significance with SBI or CMBs. In our data, ESR were closely related to age, sex, diabetes, hyperlipidemia, current smoking, systolic and diastolic blood pressure, and high-sensitivity C-reactive protein.
Conclusion
High ESR was associated with larger WMH volumes in a healthy population. Since this close association was not seen in SBI or CMBs, WMH may be more related to inflammation-related pathologies.
INTRODUCTION
Cerebral small vessel disease (cSVD) is a subclinical pathology, often found in the elderly.1,2 Although cSVDs themselves are asymptomatic, they are clinically important because they increase the risk of ischemic stroke or vascular dementia.3-5 There are subtypes with various pathologies (e.g., white matter hyperintensity [WMH], silent brain infarct [SBI], and cerebral microbleeds [CMBs]) in cSVD. These cSVD subtypes are very different in appearance, but are often found together in brain magnetic resonance imaging (MRI).1,6 In addition, previous autopsy studies have also found a link between them.2,7 Therefore, many studies have been conducted to find the common pathological mechanisms shared between them. Various mechanisms have been proposed as hypotheses, and subclinical inflammation is one of them.7-10
Erythrocyte sedimentation rate (ESR) is an index that reflects the aggregation of red blood cells, and is accelerated by the asymmetry of charged proteins (e.g., fibrinogen, immunoglobulin, lipoprotein) accompanying the occurrence of inflammation.11,12 Since ESR is an inexpensive, validated, and generally available test, it has long been used as a nonspecific inflammatory marker.11-13 In addition, ESR, like other inflammatory markers, has been closely associated with various metabolic diseases, atherosclerosis, cardiovascular diseases, and cerebrovascular diseases.14-18 It is thought that ESR will also have a close relationship with cSVD, which shares similar pathologies with these, but study on this has not been done yet.
In this study, we aimed to evaluate the relationship between ESR and cSVD in a neurologically healthy population. In addition, through comparisons between cSVD subtypes, we would like to examine whether ESR is involved in the common pathological mechanisms of cSVD development or whether it is more closely related to a specific cSVD subtype.
SUBJECTS AND METHODS
1. Study population
From a consecutive registry at a large medical center in Korea (Seoul National University Hospital Health Promotion Center), we included participants who visited to conduct a voluntary routine health check-up, between January 2006 and December 2013.19 Then, we additionally excluded participants with the following conditions: 1) age under 30 years, 2) history of stroke or severe neurological deficit, 3) hemato-oncologic conditions or use of immunosuppressant, 4) having major surgery or severe trauma, 5) severe hepatic or renal disease, or 6) active infection within prior 2 weeks.19 Finally, a total of 2,553 subjects were included in the final analysis.
This study was approved by the Institutional Review Board (IRB) of the Seoul National University Hospital (IRB No. 1502-026-647). The requirement to obtain informed consent from participants was waived by the IRB due to the retrospective study design using de-identified information. All experiments were performed in accordance with the Declaration of Helsinki and relevant guidelines and regulations.
2. Demographic, clinical, and laboratory assessments
We conducted broad evaluations including age, sex, hypertension (using anti-hypertensive agents, or ≥140 mmHg systolic blood pressure [BP], or ≥90 mmHg diastolic BP), diabetes (using glucose-lowering agents, or ≥6.5% hemoglobin A1c levels), hyperlipidemia (using lipid-lowering agents, or ≥240 mg/dL total cholesterol levels), ischemic heart disease, current smoking, systolic and diastolic BP, and use of anti-platelet agents.19 Blood pressure was checked after 5 minutes rest in sitting position. Laboratory examinations were conducted on the same day after 12 hours of overnight fasting, including glucose profiles, lipid profiles, white blood cell (WBC) counts, high-sensitivity C-reactive protein (hsCRP) and ESR.19
3. Radiological assessments
All participants underwent brain MRI and MRA using 1.5-T MR scanners (Signa, GE Healthcare, Milwaukee, WI, or Magnetom SONATA, Siemens, Munich, Germany). The detailed acquisitions of MRI were as follows: T1-weighted images (repetition time [TR]/echo time [TE]=500/11 ms), T2-weighted images (TR/TE=5,000/127 ms), T2-gradient echo images (TR/TE=57/20 ms), T2 fluid-attenuated inversion recovery images (TR/TE=8,800/127 ms), and three-dimensional time of flight MRA images (TR/TE=24/3.5 ms, slice thickness=1.2 mm). The slice thickness was 5 mm, except for time of flight MRA images.
As subtypes of cSVD lesions, we measured WMH volumes and the presence of SBI and CMBs. WMH volumes were rated quantitatively using Medical Imaging Processing, Analysis, and Visualization (MIPAV, version 7.3.0, National Institutes of Health, Bethesda, MD, USA).19 In this process, we used a computer-assisted semi-automated technique, measuring from converted DICOM files, as in our previous studies.19,20 SBI was defined as an asymptomatic and well-defined lesion larger than 3 mm in size, with signal characteristics same as those of the cerebrospinal fluid on T1- or T2-weighted images.1 CMBs were defined as focal round lesions less than 10 mm in size with low signal on T2-gradient echo images.1 All radiological parameters were rated by two neurologists (K.W.N. and H.Y.J.), and disagreements were resolved by discussion with a third rater (H.M.K.).
4. Statistical analysis
All statistical analyses were performed using SPSS version 20.0 (IBM Corp., Armonk, NY, USA). Univariate linear regression analyses were conducted to identify possible predictors for WMH volumes. Continuous variables with skewed data were transformed into a squared root scale, including WMH volumes. Then, variables with p<0.10 were introduced into the multivariable linear regression analysis along with age and sex as confounders. Since SBI and CMBs are binary outcome variables, we used multivariable logistic regression analyses for both. In addition, we investigated the relationship between ESR and demographic, clinical, and laboratory parameters in order to understand the characteristics of subjects with high ESR. For this analysis, we used a simple linear regression analysis. All variables with a p<0.05 were considered statistically significant in this study.
RESULTS
A total of 2,553 participants were evaluated (mean age: 57±10 years, male sex: 54%). The mean WMH volumes were 2.53±6.06 mL. SBI and CMB were found in 193 (7.6%) and 108 (4.2%), respectively. The mean ESR was 12±13 mm/hour. Other detailed baseline characteristics are shown in Table 1.
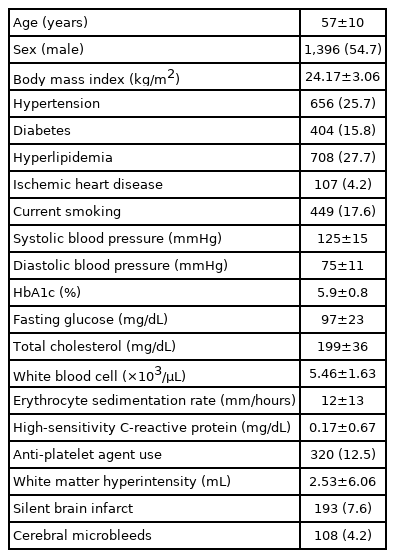
Baseline characteristics (total n=2,553)
In univariate linear regression analysis, WMH volumes were significantly associated with age, hypertension, diabetes, hyperlipidemia, current smoking, systolic and diastolic BP, hemoglobin A1c levels, fasting glucose levels, total cholesterol levels, WBC counts, ESR, and use of anti-platelet agents (Table 2).

Univariate linear regression analysis between white matter hyperintensity volume and demographic, clinical, laboratory, and radiological factors
In multivariable linear regression analysis, ESR (β=0.027, 95% confidence interval [CI]=0.001 to 0.053, p=0.043) showed significant association with WMH volumes after adjusting for confounders. Age (β=0.046, 95% CI=0.042 to 0.051, p<0.001), hypertension (β=0.187, 95% CI=0.092 to 0.281, p<0.001), and WBC counts (β=0.042, 95% CI=0.018 to 0.067, p=0.001) were also significantly associated with WMH volumes, being independent from ESR (Table 3). On the other hand, neither SBI nor CMBs showed statistical significance with ESR (Supplementary Table 1).
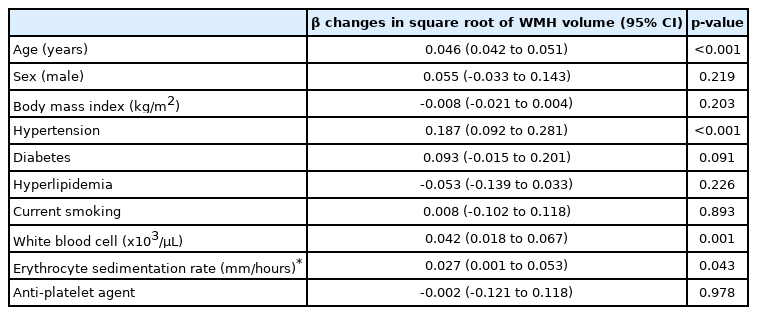
Multivariate linear regression analysis of possible predictors for white matter hyperintensity volume
In our data, ESR were associated with older age, female sex, diabetes, hyperlipidemia, current smoking, diastolic BP, hemoglobin A1c level, fasting glucose level, total cholesterol level, and hs-CRP level (Table 4).

Univariate linear regression analysis between erythrocyte sedimentation rate and demographic, clinical, and laboratory parameters
DISCUSSION
In this study, we found that high ESR were associated with larger WMH volumes in a healthy population. In addition, WMH volume was closely related to WBC counts, and ESR was not statistically significant with SBI and CMBs. Given these findings, WMH appears to be more closely related to inflammatory pathology than other cSVD subtypes.
The exact mechanisms explaining the close relationship between ESR and WMH volume are unclear. However, we suggested several plausible hypotheses. First, it may be due to the destruction of the blood-brain barrier (BBB) by endothelial dysfunction. Inflammatory cytokines and reactive oxygen species arising from subclinical inflammation conditions can interfere with the secretion of nitric oxide by endothelial cells.19,21 Alternatively, the BBB itself may be mechanically damaged by an upregulated inflammatory cascade.19,22 Damaged BBB, functionally or mechanically, causes periventricular infiltration of several toxic materials (e.g., protease, immunoglobulin, and complement components), and can cause WMH by damaging the surrounding neural tissues.8,19,23 In addition, damaged BBB can prevent clearance of interstitial fluid through the glymphatic pathway, which can also lead to WMH.1,19 In our data, not only ESR but also elevated WBC counts showed a positive correlation with WMH volume, so this hypothesis seems valid. Second, chronic diffuse hypoperfusion may have been involved. The aforementioned decrease in nitric oxide production of endothelium can also decrease the ability to control cerebral perfusion through autoregulation.23,24 In addition, subclinical inflammation may prevent the proliferation of vascular smooth muscle cells and proceeds to fibrosis, causing atherosclerosis of small arterioles permanently.23,25,26 This is evidenced by several results showing that ESR is closely related to arterial stiffness in previous studies.15 In addition to small vessels, ESR has been shown to be closely correlated with atherosclerosis of large vessels.11,12 Chronic diffuse hypoperfusion caused by the stenosis of such large and small vessels is sufficient to grow WMH volumes. Last, it may simply be the result of ESR and WMH sharing multiple risk factors. Of course, subclinical inflammation is known to be closely related to several metabolic diseases.27 However, in our data, ESR showed a close correlation with older age, diabetes, hyperlipidemia, high BP, hs-CRP level, but not with WBC counts. Therefore, although it has not yet been identified, there may be a link between them through pathway other than the inflammation.
Interestingly, ESR showed a close association only with WMH and no statistical significance with SBI or CMBs. This phenomenon is interpreted as the fact that other pathological mechanisms unrelated to subclinical inflammation and endothelial dysfunction play many roles in the development of SBI and CMBs. In addition to lipohyalinosis, it is known that embolism caused by proximal sources and microatheroma are involved in SBI development.3,7 In case of CMBs, lobar and deep CMBs are caused by different mechanisms, and hypertensive insult or amyloid angiopathy can affect this.1,6 However, in addition to differences in mechanisms, these statistical results may have arisen due to the unusually low prevalence of SBI and CMBs in our young and healthy study population.
There are several caveats to interpret our results. First, this study is a retrospective cross-sectional design. Therefore, we can only prove the association between the ESR and the WMH volume, not the causal relationship. For this, further prospective study is needed. Second, we conducted a study on a relatively young and healthy population. Thus, the influence of age and various vascular risk factors may have been relatively underestimated, and the influence of ESR may have been overestimated. Third, in order to accurately measure the WMH volume, the whole brain volume should have been measured as well. By standardizing on the basis of the ratio between the two, it was possible to minimize the difference due to the head size. Fourth, ESR is a parameter that is affected by various medical conditions such as sex, obesity, menstruation, and medication. Therefore, when applied in practice, it must be judged comprehensively with the clinical situation or other biomarkers. Last, we measured the periventricular WMH and subcortical WMH together when rating the WMH volumes. In previous studies, different mechanisms and characteristics have been reported between the two areas of WMH.28 Due to technical limitations, this study could not separate the two. Interesting results can be obtained if we can examine the relationship between ESR and WMH in the periventricular and subcortical areas respectively.
In conclusion, we demonstrated that ESR was closely related to WMH volume in a healthy population. If we classify high-risk groups through ESR and manage each of them appropriately, it may be helpful in preventing the development of WMH. By doing so, we will be able to prevent the occurrence of several neurological disorders in the subclinical stage before symptoms develop. However, our findings are needed to be validated in further prospective studies.
Supplementary Material
Supplementary Table 1.
Multivariable logistic regression analysis of possible predictors for silent brain infarct and cerebral microbleeds
Notes
Conflicts of Interest
No potential conflicts of interest relevant to this article was reported.