Relationship between Successful Cervical Carotid Stent Expansion and Low Levels of Serum Vitamin D
Article information

Abstract
Background
Serum vitamin D levels affect atherosclerosis development via diverse molecular mechanisms. The lesion characteristics of carotid stenosis affect the success of stent expansion. By comparing the pre-and post-stenting stenosis degrees, our study evaluated whether serum vitamin D levels are associated with the expansion rate of carotid stenting.
Methods
Forty-six cases who underwent elective cervical carotid artery stenting were analyzed. Patients were classified into two groups according to serum total 25-hydroxy vitamin D (25[OH]D) levels; <15.1 and ≥15.1 ng/mL. The degree of stenosis before and after stent insertion was calculated using the North American Symptomatic Carotid Endarterectomy Trial (NASCET) method. The stent expansion rate was calculated as follows: (1-[post-stent stenosis degree/pre-stent stenosis degree])×100 (%). To identify the independent factors for successful stent expansion, multivariable logistic regression analysis was conducted.
Results
Among the 46 patients, 25 (54.3%) had low serum 25(OH)D levels. The successful stent expansion rate was significantly higher in the low 25(OH)D level group (48.0% vs. 19.0%, respectively; p=0.04). In multivariable analysis, after adjusting for possible covariates, a low serum 25(OH)D level was independently associated with successful stent expansion (adjusted odds ratio, 6.47; 95% confidence interval, 1.11-37.80).
Conclusion
Low serum vitamin D levels were independently associated with successful carotid stent expansion. This study presents a new perception of biomarkers that should be considered for satisfactory carotid artery stenting.
INTRODUCTION
Vitamin D is an endogenously synthesized hormone which plays multiple roles in the immune and endocrine systems,1 in addition to its role in regulating mineral metabolism in the skeletal system. Many studies have been conducted to understand its effects on atherosclerosis in coronary and cerebrovascular diseases. As an active metabolite, 25-hydroxy vitamin D (25[OH]D) originally exerts a protective effect on vascular endothelial stability.2 However, both vitamin D deficiency and excess can exacerbate atherosclerosis via various molecular mechanisms.3
Through decades of trials, carotid artery stenting (CAS) has been recognized as a reasonable treatment option in carotid stenosis compared with carotid endarterectomy.4 Since residual stenosis impedes favorable periprocedural outcomes and long-term efficacy,5 ensuring sufficient balloon angioplasty and stent expansion is of great importance to neurointerventionists. Considering the role of vitamin D in the development of atherosclerosis, we examined whether serum 25(OH) D level influences the expansion rate of the carotid stent.
SUBJECTS AND METHODS
1. Patient and data collection
From May 2018 to June 2021, data on 78 cases of elective cervical CAS performed in Korea University Guro Hospital were retrospectively collected from the Korea University Stroke Registry (KUSR). The KUSR has been used in several research papers published in authorized journals.6-8 Among 78 cases, 32 patients with absent laboratory results were excluded. Laboratory tests included low-density lipoprotein (LDL) cholesterol, hemoglobin A1c, creatinine, C-reactive protein (CRP), D-dimer, total serum calcium, serum phosphate, parathyroid hormone, and 25(OH)D. All laboratory tests were performed within a month of stent insertion. Data on balloon diameter, number of angioplasties, types of stents, and stent diameter were collected. The balloon diameter was averaged for the multiple angioplasty cases. Stent types were divided into closed and open-cell stents. The stent diameter was averaged for the tapered stent cases.
In Korea University Guro Hospital, elective cervical CAS is suggested when the patient has stenosis of 70% or more, or an ulcerative plaque as indicated in computed tomography angiography (CTA), magnetic resonance angiography (MRA) or digital subtraction angiography (DSA); stenosis is determined as being symptomatic,9 and aspirin 100 mg or more and clopidogrel 75 mg or more is administered at least 7 days before CAS.10 The procedures for our cases were conducted when all indications were fulfilled and performed by a neuro-interventionist with over 15 years of experience. All CAS procedures were performed after obtaining informed consent.
2. Definitions and interpretation
The investigators defined a case as symptomatic when transient ischemic attack (TIA), monocular blindness, and cerebral infarction occurred ipsilateral to the stenosed target carotid artery,11 and assessment of relevance between carotid stenosis and symptoms was conducted in the Department of Neurology. A low serum level of 25(OH)D was specified by levels under 15.1 ng/mL.12 The cervical carotid artery was specified as the region of the artery running from the common carotid artery to the cervical portion of the internal carotid artery as seen in CTA, MRA, or DSA. The stenosis degree before and after stent insertion was calculated as the ratio of the diameter of the plaque measured at the most stenosed point to the distal normal luminal diameter, which is the North American Symptomatic Carotid Endarterectomy Trial (NASCET) method,13 in DSA. We defined the stent expansion rate using the following equation: (1-[post-stent stenosis degree/pre-stent stenosis degree])×100 (%). Successful stent expansion was specified as a stent expansion rate of 70% or more in DSA.14 All image assessments were performed by two neurointerventionists (J.H., H.J.) with substantial consistency (Cohen’s κ=0.83).
3. Statistical analysis
Baseline demographic, laboratory, and imaging data of the two groups were compared according to serum 25(OH)D levels, above or below 15.1 ng/mL. To search for independent factors for successful stent expansion, multivariable logistic regression analysis was conducted with variables that were assumed to be clinically relevant by investigators, or which had a p-value of less than 0.1 in comparison to baseline characteristics. Age, smoking status, hypertension, dyslipidemia, and diabetes mellitus, which are regarded as traditional risk factors for carotid stenosis, as well as the initial carotid stenosis degree, were included in the regression analysis according to the researchers’ agreement. Male sex15 and the serum levels of D-dimer,16 CRP,17 total calcium,18 phosphate,19 and parathyroid hormone20 were included in the regression analysis according to previous studies. Continuous variables were analyzed using Student’s t-test and Mann–Whitney test, whereas the frequencies of categorical variables were compared using the χ2 test and Fisher’s exact test. Spearman’s correlation coefficient was used to determine the linear correlation between serum vitamin D level and stent expansion rate. Statistical significance was set at p<0.05. SPSS for Windows version 20.0 (SPSS Inc., Chicago, IL, USA) was used.
RESULTS
The investigators assessed the retrospective data of 46 patients. The median age was 75 years (interquartile range [IQR] 69-79), and five men (10.9%) were included. Among the 46 patients, 25 (54.3%) had low serum 25(OH) D level. Age and LDL-cholesterol levels were analyzed using the Mann–Whitney test, and the frequency of sex and smoking status were assessed using Fisher’s exact test. There was no significant difference in the baseline demographic data and pre-stent stenosis degree between the groups. The serum calcium and phosphate levels did not differ between the two groups. Of the laboratory results, the level of parathyroid hormone was significantly higher in the low 25(OH)D group (37.6±3.6 vs. 27.0±3.1, respectively; p=0.03). The successful stent expansion rate was significantly higher in the low 25(OH)D level group (48.0% vs. 19.0%, respectively; p=0.04) (Table 1). The diameter of the balloon, number of angioplasties, types of stents, and stent diameters did not differ between the groups. Serum 25(OH)D levels were negatively correlated with stent expansion rate (Spearman’s correlation coefficient =-0.34, p=0.02) (Fig. 1).

Baseline characteristics of patients
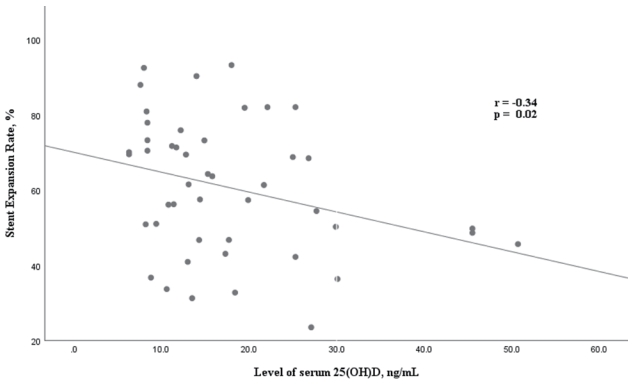
Correlation analysis using Spearman’s correlation coefficient. The level of serum vitamin D and stent expansion rate were negatively correlated.
Logistic regression analysis was performed to identify independent factors associated with successful stent expansion. Low serum 25(OH)D level was significantly related (odds ratio [OR], 3.92; 95% confidence interval [CI], 1.03-15.0), whereas parathyroid hormone level was not associated (OR, 1.01; 95% CI, 0.97-1.05) with successful stent expansion in univariate analysis. In multivariable logistic regression analysis, age, male sex, hypertension, dyslipidemia, ever smoking status, and low 25(OH) D level, pre-stent stenosis degree, and serum levels of CRP, D-dimer, total calcium, phosphate, and parathyroid hormone were included as possible covariates; low serum 25(OH)D level was independently associated with successful stent expansion rate (adjusted OR, 6.42; 95% CI, 1.09-37.7) (Table 2).
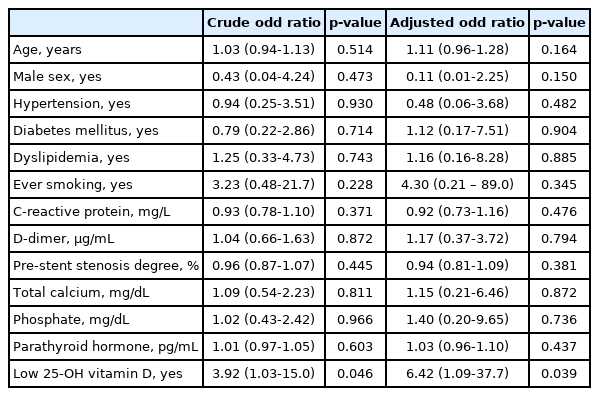
Logistic regression analysis for successful stent expansion
Two representative cases, compatible with our study results, are shown in Fig. 2. Case 1 demonstrates a patient with a successful stent expansion rate (90.3%), serum 25(OH)D level below 15.1 ng/mL (14.0 ng/mL), and a pre-stent stenosis degree of 76.1% (Fig. 2A, B). Case 2 demonstrates a patient without a successful stent expansion rate (23.5%), serum 25(OH)D level above 15.1 ng/mL (27.1 ng/mL), and a pre-stent stenosis degree of 76.9%. (Fig. 2C, D).

Two representative cases with similar pre-stenting stenosis degrees. Anterior-posterior (AP) and lateral views of the angiogram pre- and post-stenting are demonstrated. Case 1) A patient with a successful expansion rate (90.3%), serum 25-OH vitamin D level below 15.1 ng/mL (14.0 ng/mL), and a pre-stent stenosis degree of 76.1%. (A) Pre-stenting AP and lateral views and (B) post-stenting AP and lateral views in the angiogram, respectively. Case 2) A patient without a successful expansion rate (23.5%), serum 25-OH vitamin D level above 15.1 ng/mL (27.1 ng/mL), and a pre-stent stenosis degree of 76.9%. (C) Pre-stenting AP and lateral views and (D) post-stenting AP and lateral views in the angiogram, respectively.
DISCUSSION
In summary, among the baseline characteristics, the rate of successful stent expansion showed a significant difference between the low- and high-vitamin D groups. In the multivariate logistic regression analysis, low vitamin D levels were independently associated with successful stent expansion.
In the past 20 years, plaque composition has emerged as a major influential factor in determining whether coronary or carotid stenosis exerts a hazardous effect on disease prognosis. The histologic features of unstable plaques include intraplaque hemorrhage, a lipid-rich necrotic core, and a thin fibrous cap.21 In contrast to the latter, mature stage of atherosclerosis with more fibrotic, calcified lesions in “soft” plaques are related to early stage atherosclerosis.22 With larger neointimal and plaque areas, unstable plaques are susceptible to arterial remodeling, and are associated with in-stent restenosis,23 plaque fragmentation, and embolism.24 In this manner, unstable carotid plaques increase the ipsilateral stroke by 4- to 12-times independent of the degree of stenosis.25
A recent study revealed that low vitamin D levels make carotid plaques vulnerable by inducing intraplaque hemorrhage.26 At low vitamin D levels, the local angiotensin system loses inhibition and becomes abnormally activated, resulting in microvascular leakage and inflammation.27 However, the mechanically soft nature of unstable plaques was related to greater luminal gain after coronary stenting than calcified, stable plaques.28,29 In this context, the plaque characteristics in the low vitamin D group of our study could be more vulnerable and soft, thus exhibiting more successful stent expansion than in the high vitamin D group. Although reducing the degree of residual stenosis is crucial for the prognosis of CAS,5 the possibility of an underlying harmful pathology should not be neglected.
Conversely, high vitamin D levels are associated with vascular calcification by promoting vascular osteogenesis and mineralization.30 Since calcification reduces vascular stretch capacity and decreases luminal gain after CAS,31 the high vitamin D group in our study might have less successful stent expansion.
Our study had several limitations. First, this was a single-center cross-sectional study with a limited sample size. However, most cases were consecutively collected with the preinvestigated vitamin D levels. Second, there has been a lack of investigation into the determinants of vitamin D concentration. For example, variables such as supplementary vitamin D intake may prevent serum levels from reflecting the patient’s exact physiological condition. Third, a detailed evaluation of plaque characteristics was not performed using appropriate methods, such as ultrasound or high-resolution magnetic resonance imaging. A larger prospective study with additional analyses that can compensate for the limitations mentioned above is warranted to understand the effect of vitamin D on prognosis after cervical CAS.
Low vitamin D levels were independently associated with successful carotid stent expansion. Our study suggests that the serum vitamin D level could be a biomarker for satisfactory carotid artery stenting.
Notes
Ethics statement
The study protocol was approved by the Institutional Review Board (IRB) of Korea University Medical Center, Guro Hospital (IRB No. 2011GR0218). The requirement for informed consent was waived.
Availability of Data and Material
The data that support the findings of this study are available in the text.
Sources of Funding
This research was supported by an R&D support grant (K2108031) from the Korea University Guro Hospital, Republic of Korea.
Conflicts of Interest
No potential conflicts of interest relevant to this article was reported.
Acknowledgements
None.