Increased Risk of Intracranial Hemorrhage and Mortality Following Thrombolysis in Patients with Stroke and Active Cancer
Article information
Abstract
Background
The cerebrovascular disease is not uncommon in cancer patients. However, the effectiveness and safety of thrombolysis for acute ischemic stroke in this patient group has not been established well. We aimed to investigate the outcomes of thrombolysis for the patients suffering from cancer.
Methods
We conducted a retrospective analysis using database of patients who had received thrombolysis in two university hospitals. Included patients were those who had received intravenous thrombolysis or endovascular therapy. We compared mortality, and the incidence of hemorrhagic transformation (HT) and symptomatic intracerebral hemorrhage (sICH) between patients with active cancer and those without.
Results
Among a total of 627 patients, 42 (6.7%) had a medical history of active cancer. The mortality was higher in cancer patients than the others (27.5% vs. 13.7%, p=0.023). The existence of cancer was one of the factors to increases the risk of mortality (adjusted odds ratio, 3.354; 95% confidence interval, 1.416-7.947; p=0.006). From the 240 patients treated with intravenous thrombolysis only, the incidence of HT (53.8% vs. 16.3%, p=0.003), sICH (30.8% vs. 2.2%, p=0.001), and mortality (41.7% vs. 8.1%, p=0.003) was higher in cancer patients than the patients without.
Conclusion
Comorbidity with cancer raised the risk of mortality in patients when treated with thrombolysis. The patients with cancer had more bad outcomes with intravenous thrombolysis only. Our data suggest that the decision of thrombolytic treatment for cancer patients requires careful consideration.
INTRODUCTION
Previous researches conducting autopsy for the patients with cancers reported some evidences that cerebrovascular disease was found in 7.4-15% [1,2]. The factors leading to the cerebrovascular disease in these patients include coagulopathy or tumor embolism associated with cancers [3], although hypertension, diabetes mellitus, hyperlipidemia, smoking, and atrial fibrillation also play roles in stroke development [4].
Intravenous (IV) recombinant tissue plasminogen activator (rt-PA) have been used as the only approved treatment of hyperacute ischemic stroke since 1995 [5], and endovascular therapy using stentriever has been approved since 2015 [6].
Nevertheless, the effectiveness and safety of thrombolysis treatment was not precisely evaluated for the patients with cancers. Case series [7-9] and retrospective analysis with small number of patients reported the safety of thrombolysis in cancer patients [10,11]. There was few researches have been conducted on the clinical outcome of active cancer patients received thrombolysis. Hence, we investigated the outcome of the patients suffering from cancers who received thrombolysis.
SUBJECTS AND METHODS
1. Patient selection
After approval from the Institutional Review Board of Gangnam Severance Hospital and Severance Hospital, we retrospectively selected the patients with acute ischemic stroke from our stroke registry between January 2006 and August 2013 including all consecutive patients admitted to our two tertiary hospitals. Inclusion criteria were: 1) the patients who received IV rt-PA, 2) who underwent the diagnostic work-up to reveal etiology for stroke including cardioembolic source, 3) who performed the follow up imaging study after thrombolysis. 4) The presence of active cancer was identified by checking the medical records. And 5) the patients who diagnosed as active cancer during the hospitalization for acute ischemic strokes. The patients with active cancer were defined as those who were diagnosed during the stroke admission or who had stroke onset in the course of cancer treatment. IV rt-PA was given only to the patients within 3 hours of symptom onset. The endovascular therapy was performed contiguously in the patients who had no significant improvement of neurologic deficit after IV thrombolysis within 6 hours of symptom onset. Patients transferred to other hospitals after thrombolysis were excluded from the study (Fig. 1). Patients with brain tumor did not receive thrombolysis. No patient with active cancer received irradiation to the head and neck area, and none had cerebral metastasis. The patients who currently showed no evidence of cancer after receiving all planned treatment 5 years ago were classified as general patients.
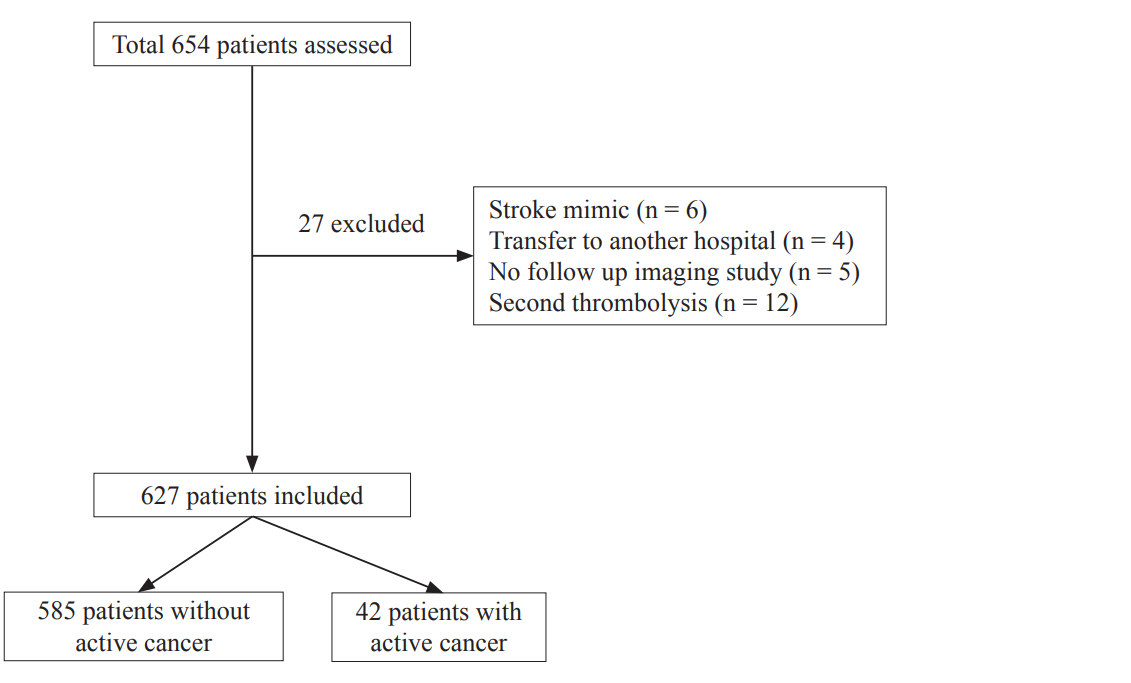
Flow chart of enrollment (inclusion and exclusion).
2. Evaluation of clinical outcome and risk factors during follow-up period
Neurologic deficit was assessed with the National Institutes of Health Stroke Scale (NIHSS) at admission, every 2 hours within 1 day, and twice a day within 3 days after symptom onset. Prognosis of patient was evaluated by using the 3 months modified Rankin scale (mRS). Favorable outcome was defined as mRS ≤2. Brain computed tomography (CT) or magnetic resonance imaging (MRI) was conducted to check presence of cerebral hemorrhage or progression of cerebral infarction within 36 hours.
Presence of hemorrhagic transformation (HT) was determined by using brain CT or gradient echo MRI. Symptomatic intracerebral hemorrhage (sICH) was defined as any type of hemorrhage accompanied by more than 4 point increment of NIHSS score [12]. Based on the reviews of clinical charts and test results, this study examined the factors which can affect the prognosis, the factors which are known to be associated with HT, and the conventional risk factors of ischemic stroke.
3. Statistical analysis
This study used SPSS version 20.0 (SPSS Inc., Chicago, IL, USA) for windows for statistical analysis. In order to examine the difference in demographic data, student’s t-test was used for continuous variables, and chi-square was used for categorical variables. Logistic regression analysis was used to examine independent factors affecting sICH and mortality stepwise method was used for the selection of variables. Chi-square test was used to examine the difference in incidence of HT or sICH according to presence of cancer in the patients who had received IV rt-PA. The level of statistical significance was set to p<0.05.
RESULTS
Of the total 627 patients, 42 patients (6.7%) had the medical history of active cancer (Fig. 1). A total of 531 including 40 patients with active cancer were available for follow-up until three months. Ten patients had colorectal cancer, eight patients had gastric cancer, six patients had lung cancer, five patients had hepatobiliary cancer, four patients had pancreatic cancer, three patients had prostate cancer, three patients had leukemia, two patients had cervical cancer, and one patient had endometrial cancer.
Diabetes mellitus was more prevalent in patients with active cancer and high-risk potential cardiac sources of embolism including atrial fibrillation were more prevalent in patient without active cancer. Glucose, hemoglobin, hematocrit and platelet count showed significant difference between the two groups. In addition, the patients with active cancer showed lower initial systolic and diastolic blood pressure (Table 1).

Baseline demographic data between two groups
There was no difference in the occurrence of HT and sICH. After 3 months of follow up, there was no difference in the favorable outcome between the patients with and without active cancer. However, mortality was significantly higher in patients with active cancer than the others (27.5% vs. 13.7%, p=0.023) (Table 1). Fifty-seven patients (9.1%), including four active cancer patients, were discharged with death. Two patients with active cancer died for other reasons than ischemic stroke and thrombolysis related problems. And two patients died due to systemic bleeding.
The undetermined etiology were classified as cryptogenic stroke. When we compared the combined group of cardiogenic embolism (CE) and cryptogenic stroke with patients of large artery atherosclerosis (LAA), the etiology of cerebral infarction and sICH tended to be related (p=0.056). However, the etiology and mortality were not related (p=0.143). When cryptogenic stroke was compared with conventional causes including CE and LAA, the etiology and sICH were not related (p=0.165). The factors significantly related to the risk of sICH for the total patients were the existence of diabetics and initial NIHSS (Table 2). The factors significantly related to the mortality were the sICH, active cancer and initial NIHSS (Table 3).
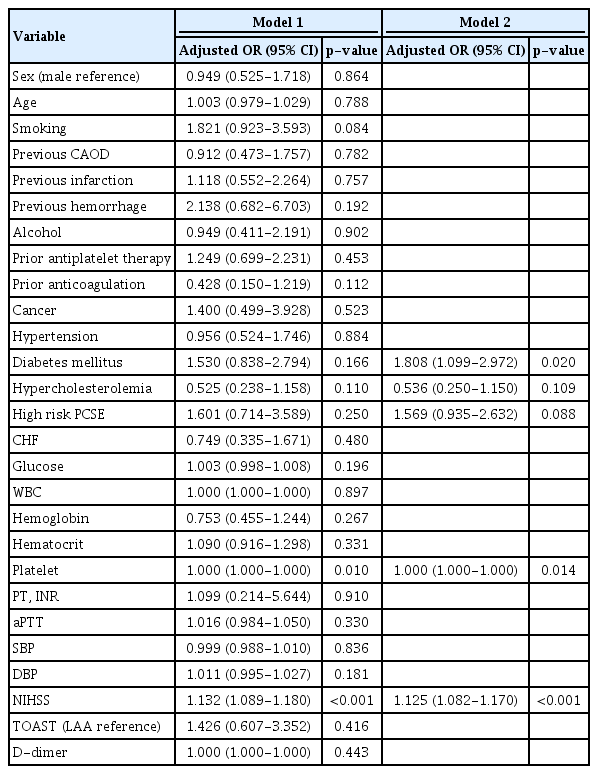
Logistic regression model of factors independently associated with symptomatic ICH

Logistic regression model of factors independently associated with mortality
Among the 240 patients who used only IV rt-PA, 13 patients (5.4%) had the medical history of active cancer (Table 4). There was no difference in the conventional risk factors of ischemic stroke, except atrial fibrillation between the two groups. The patients received only IV thrombolysis with active cancer showed more HT (53.8% vs. 16.3%, p=0.003), sICH (30.8% vs. 2.2%, p=0.001), and higher mortality (41.7% vs. 8.1%, p=0.003) than those without active cancer.
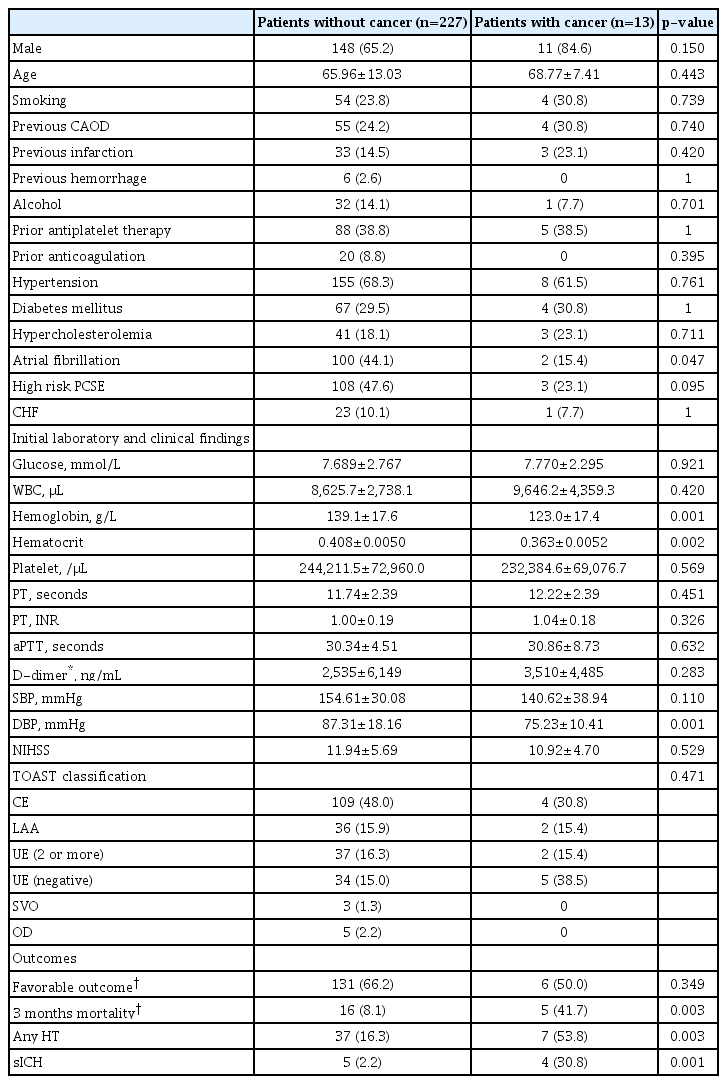
Baseline demographic data, clinical characteristics, and outcomes of patients receiving IV rt-PA
In the logistic regression analysis about thrombolysis methods depending on the existence of active cancer, use of rt-PA significantly increases the risk of HT for the patients with active cancer about 3.14 times more than that of the patients without active cancer (p=0.01). It also increased the risk of sICH about 3.98 times more (p=0.02) and risk of mortality about 6.07 times more (p=0.001). Endovascular therapy did not increase the risk of HT, sICH, and mortality. This is an example image of a representative patient with sICH after thrombolysis (Fig. 2).
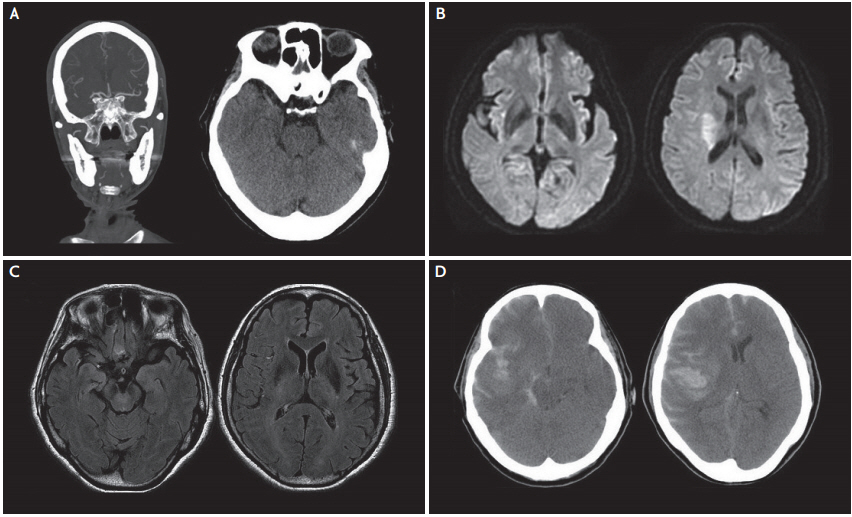
A 67-year-old woman with lung cancer was treated by intravenous thrombolysis and endovascular therapy. (A) Brain CT angiography shows occlusion of right MCA and brain CT shows hyperdense sign. (B) Diffusion MRI shows acute infarction in a part of the right MCA territory. (C) FLAIR MRI does not show significant signal change yet. (D) Brain CT obtained after 6 hours of treatment shows cerebral hemorrhage. CT; computed tomography, MCA; middle cerebral artery, MRI; magnetic resonance imaging, FLAIR; fluid attenuated inversion recovery.
DISCUSSION
This study showed the incidence of mortality within 3 months is significantly higher in patients with active cancer after thrombolysis. However, there was no difference on the sICH and favorable outcome after 3 months between those with and without active cancer. Among the patients had received only IV thrombolysis, the incidence of HT, sICH, and mortality within 3 months were all significantly higher in patients with active cancer.
The mortality was higher in the patients with active cancer than those without active cancer in this study. This study analyzed the factors associated with sICH and mortality respectively. The factors related to the risk of sICH were diabetes mellitus and initial NIHSS which were similar to that of previous reports [13]. The most significant factor associated with mortality was sICH and it was similar results like another study [14]. A meta-analysis also reported that sICH is correlated with mortality [15]. Initial NIHSS were also reported as an independent predictor of death after thrombolysis [16]. Subtherapeutic international normalized ratio (INR) in patients using warfarin increases the risk for sICH after thrombolysis [17]. Previous meta-analysis revealed that use of warfarin did not increase mortality in patients received thrombolysis [18]. However, 11% of patients were used warfarin before thrombolysis in this study. Therefore, there may be differences in results from previous studies. Presence of active cancer was also significant factor associated with mortality. One of the reasons is the death from complications associated with cancer itself. Secondly, systemic bleeding was the cause of death in active cancer patients. Although the two studies were based on the long-term follow up results, patients comorbid with cancer were associated with higher mortality among the ischemic stroke patients [19,20].
In active cancer patients, the risk of HT, sICH and mortality were all increased with the use of rt-PA, not by endovascular therapy. Analyzing the patients who received IV thrombolysis only, not only the mortality rate in patients with active cancer, the proportion of cerebral hemorrhage were also higher than the patients without cancer. The mechanical device and urokinase are both used for the localized endovascular therapy. However, IV rt-PA acts systemically on the whole body system, and systemic coagulopathy resulting bleeding complication was often accompanied in cancer patients [21]. It may have made the difference in the bleeding tendency between the patients with active cancer and those without. Probability of causing systemic hemorrhage by intravenous thrombolysis was only about 1% in previous studies, but they did not include the patients with cancer [5,22].
Previously, it was reported that intracranial hemorrhage is accompanied with the patients with cancer [1]. Researches had been conducted to explore the cause of this result, and they reported that coagulopathy was mainly related to the result [23]. Coagulation disorders in cancer patients is known to be caused by the tumor growth and related mechanisms [24]. The biomarkers level related coagulopathy are higher in stroke patients with cancer than those without cancer [25]. The impairments of coagulation cascade can result from hepatic failure or the deficiency of vitamin-K [26]. Even though the INR level is within the normal range, the patients with cancer are sometimes deficient in vitamin-K due to nutrient deficiency resulting from anorexia [27]. It has been also reported that a number of patients with cancer die of cerebral bleeding caused by cancer related microangiopathic hemolytic anemia [28].
The limitation of this study lies in the analysis of the combined data from the patients who had used a variety of thrombolysis methods. This study included a number of data from the patients using urokinase which is not frequently used currently. Also, the types of mechanical device used vary, depending on the time of being treated. Because, this study included old data when the mechanical thrombectomy device were not generally used. This study included a small number of various cancer patients. Therefore, it was difficult to analyze the difference in outcomes according to cancer stage. The percentage of the HT in this study was about 10% higher than that of previous studies [29,30]. And the percentage of the sICH was also about 5% higher than that of previous literatures [31]. This might result from the inclusion of patients who received various combined thrombolysis methods unlike previous studies. Another reason was that this study use not only CT scan but also MRI to detect HT. Of the total patients in this study, 512 patients performed MRI scans to verify the existence of HT after receiving thrombolysis. It has been reported that MRI is more sensitive to identify HT than CT [32]. As described above, the relatively high percentage of sICH in this study might result from the fact that this study included the patients who used various methods together. When we analyzed the patients receiving IV rt-PA only, our study showed the similar result of sICH for the patients without active cancer [15]. Recent study showed the similar rate of sICH like this study [33].
This research involved large number of patients than the previous study [10]. However, it was difficult to conduct the statistical analysis due to the small number of the patients with active cancer. Because of this, the group who used rt-PA only was the only group which could be analyzed independently by the type of treatment method. Unlike the recent studies, this study could not make a comparative analysis for the patients who used mechanical devices.
Based on the findings from this study, it is suggested that the observation of the patients who have the medical history of active cancer should be made actively and consistently when they receive the thrombolysis treatment. Especially, the use of rt-PA requires to be managed properly with careful attention of the risk of hemorrhage. And it should be considered that mortality may increase after thrombolysis in the active cancer patients. This can be supported by the evidence from prospective research which includes a larger number of patients.
Notes
Conflicts of Interest
No potential conflicts of interest relevant to this article was reported.