Reversal of a Large Ischemic Lesion with Low Apparent Diffusion Coefficient Value by Rapid Spontaneous Recanalization
Article information

Abstract
Cytotoxic edema at the site of a lesion following cerebral infarction is shown as a high signal on diffusion-weighted imaging, with a corresponding decreased apparent diffusion coefficient value on magnetic resonance imaging. These imaging findings have been used clinically as imaging markers of the infarction core, implying irreversible ischemic damage. However, reversal of diffusion lesions has been reported in patients with small lesions, relatively higher values of the apparent diffusion coefficient, or rapid endovascular reperfusion. Herein, we report a case of reversal of a large ischemic lesion on diffusion-weighted imaging with corresponding low apparent diffusion coefficient values in an acute middle cerebral artery infarction after immediate spontaneous recanalization. This case suggests that large ischemic lesions revealed by diffusion-weighted imaging may be reversed upon timely reperfusion, and could be considered as therapeutic targets.
Cytotoxic edema causes restriction of diffusion on diffusion-weighted imaging (DWI) with a corresponding decreased apparent diffusion coefficient (ADC) value, which implies pathological changes in cells in acute ischemic stroke. Clinically, these magnetic resonance imaging (MRI) findings have been thought to directly imply irreversible ischemic damage, and are used as imaging markers of the infarction core. However, the association between DWI lesions and the infarction core has been challenged in several recent case reports and systemic analysis of DWI reversal.1-3 These reversals are usually observed in patients with small lesions, relatively higher ADC values, or rapid endovascular reperfusion.3-6 Herein, we report a case of reversal of a large ischemic lesion on DWI with corresponding low ADC values in acute middle cerebral artery (MCA) infarction after immediate spontaneous recanalization.
CASE
A 76-year-old woman presented with sudden onset left-sided weakness along with hemineglect and dysarthria 6 hours prior to admission. The patient had a history of dyslipidemia, atrial flutter, and lung and sigmoid colon cancers. The initial National Institutes of Health Stroke Scale (NIHSS) score was 11. Brain computed tomography angiography performed 36 minutes after admission showed an occlusion of the proximal segment of the right MCA. DWI (b=1,000 s/mm2, TR=5,000 ms, TE=63.7 ms, slice thickness=3 mm) performed on a 3.0T MR scanner (Signa 3.0T; General Electric, Boston, MA, USA) 81 min after admission showed a lesion with high signal intensity in the right MCA territory (Fig. 1). On the ADC map, the average absolute ADC value of the lesion was 322.6×10-6 mm2/s, and the ratio of the ADC value of the ischemic hemisphere to the unaffected contralateral hemisphere was 0.52. A perfusion delay was observed in the territory corresponding to the occluded MCA. The NIHSS score improved to 5 immediately following brain MRI. Cerebral angiography 90 min after MRI showed spontaneous recanalization of the occluded right proximal MCA, with distal occlusion of the inferior division. Follow-up brain MRI performed 3 days after admission showed complete reversal of the initial high signal intensity lesion on DWI and no fluid-attenuated inversion recovery (FLAIR) signal change. Although recanalization was observed in the previously occluded inferior branch of the right MCA, new infarctions with FLAIR changes were detected in the corresponding territory (Fig. 2). The patient received anticoagulation therapy with edoxaban 60 mg once daily for secondary prevention, and no neurological sequelae were observed at discharge.
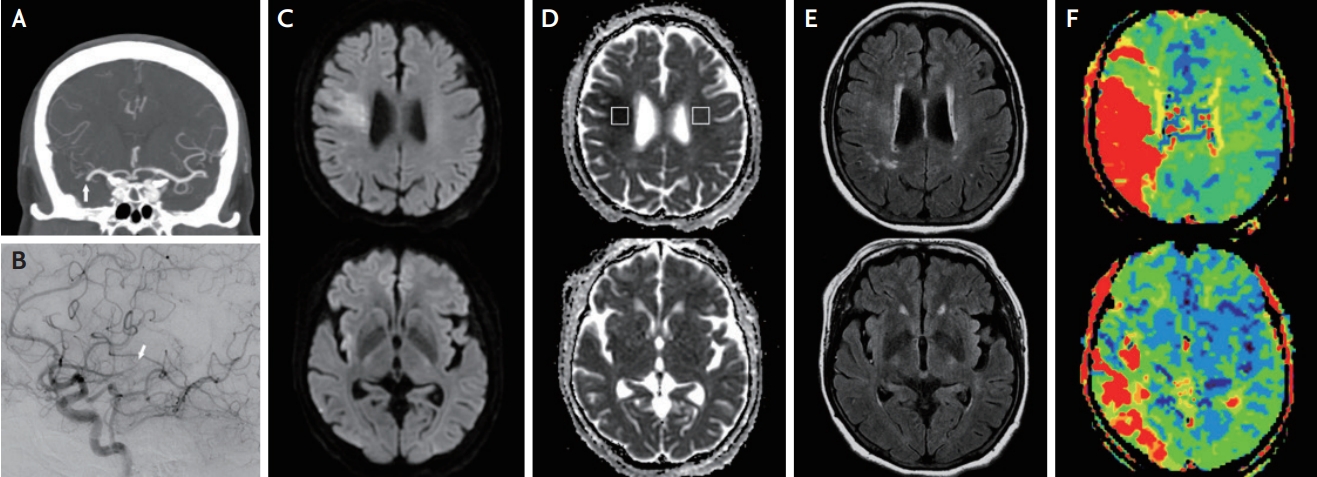
(A) Coronal brain CT angiography showing right proximal MCA occlusion (arrow). (B) Cerebral angiography showing recanalization of the right proximal MCA and occlusion of the distal inferior branch of the MCA (arrow). (C) DWI, (D) ADC map, (E) FLAIR, and (F) Time-to-peak perfusion map of brain MRI taken 7.5 hours after symptom onset showing a diffusion restricted lesion with corresponding low ADC value and perfusion delay in the right MCA territory. Average ADC value of the lesion (demarcated as a rectangle in the right hemisphere) is 322.6×10-6 mm2/s, while the average ADC value of the contralateral normal side (demarcated as rectangle in the left hemisphere) is 623.2×10-6 mm2/s. CT; computed tomography, MCA; middle cerebral artery, DWI; diffusion-weighted imaging, ADC; apparent diffusion coefficient, FLAIR; fluid-attenuated inversion recovery, MRI; magnetic resonance imaging.
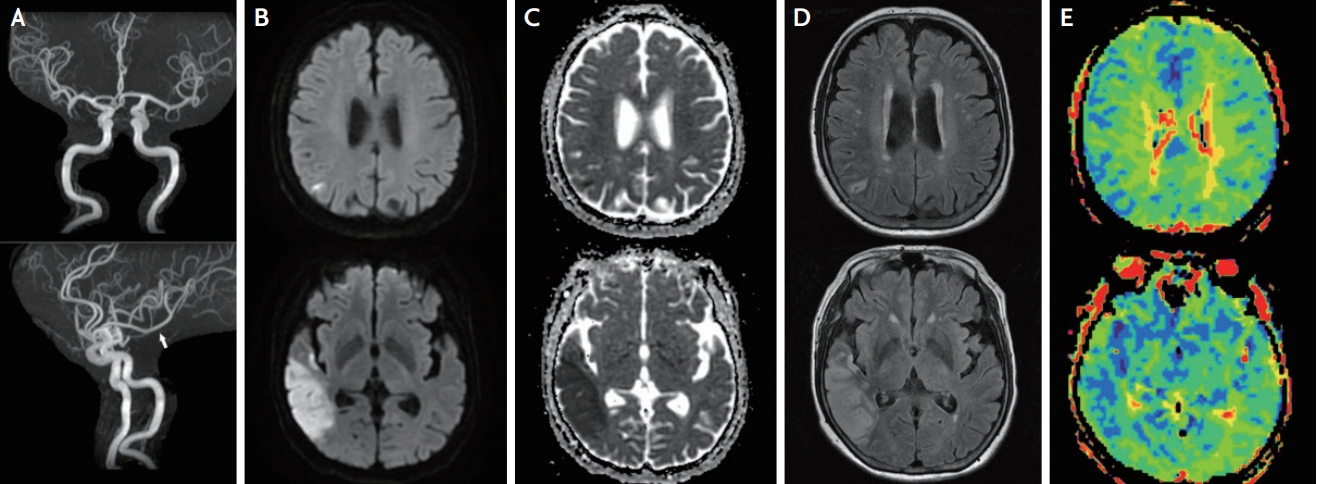
(A) Magnetic resonance angiography shows recanalization of the previously occluded inferior branch of the right MCA (arrow), (B) DWI, (C) ADC map, (D) FLAIR, and (E) Time-to-peak perfusion map of brain MRI taken 3 days later shows reversal of the initial ischemic lesion and a new lesion at the right MCA inferior division territory, with improvement of perfusion delay. MCA; middle cerebral artery, DWI; diffusion-weighted imaging, ADC; apparent diffusion coefficient, FLAIR; fluid-attenuated inversion recovery, MRI; magnetic resonance imaging.
DISCUSSION
This case showed a reversal of a large ischemic lesion, diagnosed on initial DWI and the corresponding low ADC values after early spontaneous recanalization with a new ischemic lesion on follow-up MRI caused by distal clot migration. Reduction of cerebral blood flow during a cerebral ischemic attack is thought to cause cell hypoxia and functional impairment.7 However, with timely recovery of blood flow, some of these cells may not perish and can recover normal function; this is termed “ischemic penumbra”. Since then, the clinical goal of acute ischemic stroke treatment has been to determine penumbra volume and its salvation.8,9
Cerebral edema following infarction causes a decrease in ADC value, with the degree of ADC decrease correlating with hypoperfusion and metabolic depletion of the area.7 However, previous studies focusing on the decrease in ADC value as an indicator of tissue viability mostly yielded controversial results. While a relationship between ADC decrease and lesion irreversibility has been observed, studies using ADC values as the irreversibility threshold have mostly failed.5 Besides these results, there are other proposals that ADC normalization may depend not only on the absolute value, but also on the time interval to reperfusion and final recanalization status.5,6,10 In this patient, a large ischemic lesion, defined by DWI with severely decreased ADC value, reversed after spontaneous recanalization immediately following DWI imaging. In contrast, the new ischemic lesion, which showed no diffusion restriction with significant perfusion delay on initial MRI, developed on follow-up MRI. This can be explained by the fact that prolonged ischemia in the MCA inferior division territory caused the area of the ischemic penumbra to shift into the ischemic core. This case suggests that large ischemic lesions revealed by DWI may be reversed upon timely reperfusion and may, therefore, be considered therapeutic targets.
Notes
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Severance Hospital, Yonsei University Health System (IRB No. 3-2021-0299), and the requirement for informed consent was waived.
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author upon reasonable request.
Sources of Funding
None.
Conflicts of Interest
No potential conflicts of interest relevant to this article was reported.
Acknowledgements
We would like to thank Editage (www.editage.co.kr) for English language editing.