Lower extremity peripheral arterial disease (PAD) is when the arteries in the legs and feet become narrowed and hardened, restricting blood flow. It is commonly associated with risk factors such as age, diabetes, hypertension, smoking, high cholesterol, and obesity. Lower extremity PAD is also associated with other peripheral artery diseases, such as carotid artery stenosis and coronary artery disease. Screening for lower extremity PAD is essential in assessing a patient’s risk for cardiovascular diseases. In fact, many hospitals screen for lower extremity PAD as part of a patient’s health check-up and when patients are admitted to the hospital for vascular diseases such as stroke or myocardial infarction.1
One tool commonly used to screen for lower extremity PAD is the ankle-brachial index (ABI).2,3 The ABI measures the difference in blood pressure between the arteries in the arms and legs and can be used to assess the severity of PAD. An ABI of 0.90 or less indicates a high suspicion of PAD, and an ABI of 0.50 or less indicates severe PAD. A previous study reported the ABI to be highly accurate with a sensitivity of 89%, specificity of 99%, positive predictive value of 90%, and negative predictive value of 99%.4 However, there are cases where false normalized values may occur, such as when the patient has calcification in the infrapopliteal artery or well-developed collaterals.5,6 Therefore, if a patient has vascular claudication or multiple risk factors such as advanced age, hypertension, smoking, and diabetes, it is important not to completely rule out lower extremity PAD, even if the ABI is normal. In such cases, additional tests such as lower extremity duplex ultrasound and lower extremity CT should be considered in addition to ABI to further assess the presence of PAD.
We present a case with normal ABI despite the presence of lower extremity PAD confirmed by lower extremity duplex ultrasound, lower extremity computed tomography (CT), and surgery.
CASE
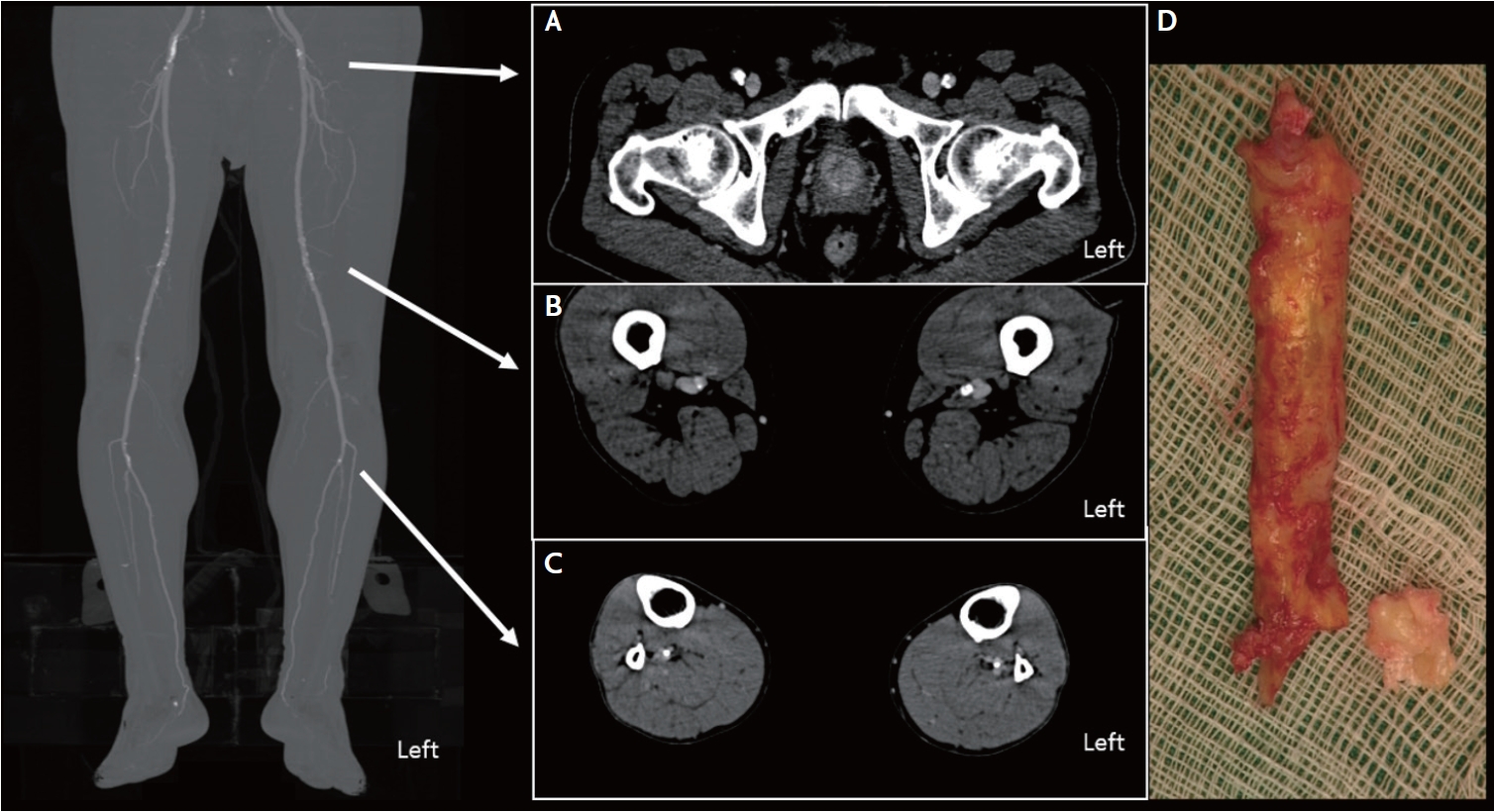
A 78-year-old male with a history of hypertension, type 2 diabetes mellitus for more than 10 years, gout, carotid atherosclerosis and subarachnoid hemorrhage presented with intermittent claudication occurring after 20 minutes of walking that began a year ago. An ABI test was performed to evaluate lower extremity PAD. The ABI was measured using a volume plethysmograph (Form PWV/ABI; Omron Health Care Co., Kyoto, Japan). The right ABI was 1.09, and the left ABI was 1.07, within the normal range (1.00–1.40). The upstroke time, the transit time from the nadir to the peak of the pulse volume waveform recording, was higher than the normal range (<180 milliseconds) in both ankles, 222 milliseconds on the right ankle and 212 milliseconds on the left ankle (Supplementary Fig. 1). During follow-up, a femoral artery duplex ultrasound was performed at another hospital. The femoral artery duplex ultrasound demonstrated a 90% or greater stenosis of the right common femoral artery. The second ABI test and a lower extremity CT were performed following the above ultrasound results. The second ABI results were also within the normal range, with 1.01 on the right and 1.05 on the left. On the second ABI, the upstroke time was normal, measuring 165 milliseconds on the right and 155 milliseconds on the left (Table 1). The lower extremity CT showed severe stenosis in the right common femoral artery with heavy calcification and moderate stenosis in the left common femoral artery. There was moderate to severe stenosis in the bilateral proximal superficial femoral arteries with calcification. The lower extremity CT also showed calcification of the bilateral proximal infrapopliteal arteries (Fig. 1A-C). However, the lower extremity CT showed no stenosis in the distal infrapopliteal artery where the ABI cuff was placed. The patient underwent endarterectomy of the right common femoral artery, and gross pathology showed near-total occlusion of the right common femoral artery with severe calcification (Fig. 1D).
DISCUSSION
An ABI test is commonly used as the initial screening test for lower extremity PAD.2,3 The accuracy of the ABI test has been well-established in previous studies.5 However, there are situations in which the ABI test may produce inaccurate results. One notable example is when there is calcification in the infrapopliteal artery that prevents complete occlusion by the air-filled blood pressure cuff.6 This condition is common in patients with diabetes, chronic kidney disease (CKD), and advanced age. In addition, falsely normalized results may occur if sufficient collateral vessels are present.5 Therefore, lower extremity PAD should not be excluded even if the ABI is within the normal range. Our patient’s ABI values were normal in the initial and subsequent ABI tests. The lower extremity CT showed stenosis with calcification in the proximal infrapopliteal artery, but no stenosis was observed around the distal infrapopliteal artery where the cuff was applied (Fig. 1C). Therefore, the falsely normalized ABI in our patient was probably not due to calcified incompressible arteries but rather to other factors such as well-developed collaterals.
If the ABI test is suspected to be falsely normalized, checking the upstroke time can be helpful for diagnosis. During the ABI testing, upstroke time is automatically measured by a volume plethysmograph. Maruhashi et al.6 reported that in cases of lower extremity PAD, the upstroke time can be prolonged even when the ABI is normal. In both cases, lower extremity CT confirmed severe calcification in the infrapopliteal artery where the ABI cuff was placed.6 Based on these findings, Maruhashi et al.6 suggested that the ABI may be falsely normalized due to calcification in the infrapopliteal artery. In contrast, the upstroke time, which is not affected by the presence of calcified incompressible arteries, may be prolonged.6 In our patient, the first upstroke time increased, with 222 milliseconds on the right side and 212 milliseconds on the left side. However, both upstroke times were within the normal range on the second ABI test (Table 1). Due to the lack of research in this area, it is currently difficult to provide a clear explanation or definitive cause for the inconsistent results observed in our patients. Further research is needed to determine the causes of these inconsistent results and to validate the importance of upstroke time.
This case demonstrates that the ABI can be falsely normalized. The ABI test can be falsely normalized in the presence of calcification in the infrapopliteal artery or when there is sufficient collateral circulation. Therefore, in the presence of risk factors such as older age, hypertension, smoking, diabetes, chronic kidney disease, or the presence of calcification in other vessels, or if PAD is clinically suspected, additional testing such as lower extremity CT or duplex ultrasound is necessary, even if the ABI test results are normal. In particular, duplex ultrasound is a simple, quick and safe method to assess PAD in the common femoral artery and superficial femoral artery.7,8